Potrebbero piacerti anche
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicDa EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicValutazione: 5 su 5 stelle5/5 (1)
- Case Presentation: Presented byDocumento34 pagineCase Presentation: Presented byZahid AnwarNessuna valutazione finora
- Case History: Personal DataDocumento5 pagineCase History: Personal DataMohammed AhmedNessuna valutazione finora
- Surgery 2 Case ReportDocumento12 pagineSurgery 2 Case ReportElvis NgNessuna valutazione finora
- Acute Appendicitis Case StudyDocumento16 pagineAcute Appendicitis Case StudyAslah NabilahNessuna valutazione finora
- Acute Appendicitis: Surgical PostingDocumento8 pagineAcute Appendicitis: Surgical PostingGraldoNessuna valutazione finora
- Case Write Up SurgeryDocumento13 pagineCase Write Up SurgerySharvin100% (3)
- Pancreatic CancerDocumento15 paginePancreatic CancerMutiana Muspita JeliNessuna valutazione finora
- Posting ElectiveDocumento7 paginePosting ElectiveThulasi tootsieNessuna valutazione finora
- Patient Profile and Appendicitis ManagementDocumento7 paginePatient Profile and Appendicitis ManagementAiman ArifinNessuna valutazione finora
- Gestational Diabetes Mellitus Induction at 40 WeeksDocumento12 pagineGestational Diabetes Mellitus Induction at 40 WeeksAiman ArifinNessuna valutazione finora
- CASE STUDY: ANAESTHESIA FOR HYSTEROSCOPYDocumento8 pagineCASE STUDY: ANAESTHESIA FOR HYSTEROSCOPYAmbhi GanaNessuna valutazione finora
- Peds Case 3Documento5 paginePeds Case 3Mohammed AhmedNessuna valutazione finora
- Pedia 1Documento8 paginePedia 1Jani MisterioNessuna valutazione finora
- Case Report, General SurgeryDocumento36 pagineCase Report, General Surgeryalnoooor38Nessuna valutazione finora
- 0 CwuDocumento7 pagine0 CwuSharvienraaj VelukumaranNessuna valutazione finora
- Acute Cholecystitis CaseDocumento16 pagineAcute Cholecystitis CaseZharif Fikri100% (3)
- Acute Appendicitis 3Documento8 pagineAcute Appendicitis 3Aiman ArifinNessuna valutazione finora
- Department of Internal Medicine: Non-Hodgkin LymphomaDocumento26 pagineDepartment of Internal Medicine: Non-Hodgkin LymphomaHana FauziNessuna valutazione finora
- Gynaecology Threatened Miscarriage Case WriteupDocumento10 pagineGynaecology Threatened Miscarriage Case WriteupGayathrie Mahalingam100% (1)
- PEDIA Case 4.1. Dengue FeverDocumento10 paginePEDIA Case 4.1. Dengue Feverotartil_nimanNessuna valutazione finora
- Case Write Up 1-CholecystitisDocumento9 pagineCase Write Up 1-CholecystitisAmbhi Gana100% (1)
- Case Write-Up 1 Obstructive Jaundice With Cholecystitis Secondary To Ampullary TumorDocumento21 pagineCase Write-Up 1 Obstructive Jaundice With Cholecystitis Secondary To Ampullary TumorwhosenahNessuna valutazione finora
- Acalculous Cholecystitis CaseDocumento35 pagineAcalculous Cholecystitis CaseSaada Enok MedtamakNessuna valutazione finora
- A Case On Periampullary Carcinoma.: Presented by DR Sumaiya Tasnim TanimaDocumento34 pagineA Case On Periampullary Carcinoma.: Presented by DR Sumaiya Tasnim TanimaJobaer MahmudNessuna valutazione finora
- Case Report LanaDocumento20 pagineCase Report Lanaboody257Nessuna valutazione finora
- Surgery Case PresentationDocumento40 pagineSurgery Case PresentationSalsabila Al-Basheer0% (2)
- Case Clerking ApendicDocumento15 pagineCase Clerking ApendicMelvin Khung100% (1)
- EM Case Write UpDocumento11 pagineEM Case Write UpRaihana Rafi100% (2)
- Gestational HypertensionDocumento71 pagineGestational HypertensionDevikha PeremelNessuna valutazione finora
- History:: Chief Complaint: History of Present IllnessDocumento4 pagineHistory:: Chief Complaint: History of Present IllnessIbrahem Y. NajjarNessuna valutazione finora
- Incomplete Abortion PanggoDocumento20 pagineIncomplete Abortion PanggoRoselle Joy D. RosalejosNessuna valutazione finora
- Name: Wong Wai Kheong Matrix No: BMS12081154Documento13 pagineName: Wong Wai Kheong Matrix No: BMS12081154myolie wuNessuna valutazione finora
- Case Base DiscussionDocumento19 pagineCase Base DiscussionNu JoeNessuna valutazione finora
- Ibn-Sina Nursing and Midwifery Collage Case Study "Nursing Management"Documento14 pagineIbn-Sina Nursing and Midwifery Collage Case Study "Nursing Management"مالك مناصرةNessuna valutazione finora
- Cwe Nephrotic SnydromeDocumento15 pagineCwe Nephrotic SnydromeFariezuan Hamid100% (1)
- Erythrodermic Psoriasis CaseDocumento8 pagineErythrodermic Psoriasis CaseMaryamNessuna valutazione finora
- Islamic University in Uganda: Habib Medical SchoolDocumento8 pagineIslamic University in Uganda: Habib Medical SchoolUsaid SulaimanNessuna valutazione finora
- Case Write Up - Harmeet - Multinodular GoitreDocumento29 pagineCase Write Up - Harmeet - Multinodular GoitreShalini Soorya71% (7)
- CP 9Documento47 pagineCP 9Mituran IshwarNessuna valutazione finora
- Farah Cwu Gynae EditDocumento16 pagineFarah Cwu Gynae EditfarahNessuna valutazione finora
- ThalassemiannDocumento62 pagineThalassemiannAndhika Hadi WirawanNessuna valutazione finora
- Cwu Surgery Y5 AsyikinDocumento21 pagineCwu Surgery Y5 AsyikinNurulasyikin MAANessuna valutazione finora
- Nursing Care Planpulmonary TuberculosisDocumento20 pagineNursing Care Planpulmonary Tuberculosisgandhialpit100% (5)
- Nakamura HX 8 Y:oDocumento8 pagineNakamura HX 8 Y:oGrachelle PiniliNessuna valutazione finora
- Clinical Case Presentation Congenital Heart DiseaseDocumento27 pagineClinical Case Presentation Congenital Heart DiseaseAdityaNessuna valutazione finora
- Case Study On Gastric Outlet ObstructionDocumento37 pagineCase Study On Gastric Outlet ObstructionJunayed Safar Mahmud100% (4)
- Surg Week 4Documento75 pagineSurg Week 4Casey YanoNessuna valutazione finora
- Foreign Body AspirationDocumento4 pagineForeign Body AspirationpriscaNessuna valutazione finora
- Diploma in Medical and Health Science Case ClerkingDocumento11 pagineDiploma in Medical and Health Science Case ClerkingWan AmeeramirulzamanNessuna valutazione finora
- Case:chronic Constrictive Pericarditis - NicvdDocumento44 pagineCase:chronic Constrictive Pericarditis - NicvdNavojit ChowdhuryNessuna valutazione finora
- HTN Complicating Pregnancy 2Documento11 pagineHTN Complicating Pregnancy 2Aiman ArifinNessuna valutazione finora
- CFGVDocumento28 pagineCFGVmyolie wuNessuna valutazione finora
- Kampala International University Western Campus Student Biodata and Medical CaseDocumento10 pagineKampala International University Western Campus Student Biodata and Medical Casefadila mohammedNessuna valutazione finora
- Case PresentationDocumento31 pagineCase PresentationArsalan NadeemNessuna valutazione finora
- Esrd FinalDocumento26 pagineEsrd FinalCreighton A. BayonganNessuna valutazione finora
- Pain Abdomen: Apurva Shrestha AampipalDocumento17 paginePain Abdomen: Apurva Shrestha AampipalApurvaNessuna valutazione finora
- Case Presentation: Muhammad Ali Bin Abdul Razak Wan Ahmad Syazani Bin Mohamed Nadiah Mohd NasirDocumento63 pagineCase Presentation: Muhammad Ali Bin Abdul Razak Wan Ahmad Syazani Bin Mohamed Nadiah Mohd NasirarbyjamesNessuna valutazione finora
- A Case Study On Pediatric Community Acquired Pneumonia-DDocumento58 pagineA Case Study On Pediatric Community Acquired Pneumonia-DAnonymous A5dkn4N3Nessuna valutazione finora
- Medicine Epilepsy ClassificationDocumento11 pagineMedicine Epilepsy Classificationismah_haron_1Nessuna valutazione finora
- Postpartum Psychiatric Disorders: By: Ismah Haron Ruzanna Rosslan Noraini TukiranDocumento7 paginePostpartum Psychiatric Disorders: By: Ismah Haron Ruzanna Rosslan Noraini Tukiranismah_haron_1Nessuna valutazione finora
- Discussion: By: Siti Nurulismah BT Che HaronDocumento18 pagineDiscussion: By: Siti Nurulismah BT Che Haronismah_haron_1Nessuna valutazione finora
- Ophthal Red Eye-conjuctivitis&SchDocumento15 pagineOphthal Red Eye-conjuctivitis&Schismah_haron_1Nessuna valutazione finora
- ENT - Anat - Oral Cavity & PharynxDocumento25 pagineENT - Anat - Oral Cavity & Pharynxismah_haron_1Nessuna valutazione finora
- PCM Family PlanningDocumento32 paginePCM Family Planningismah_haron_1Nessuna valutazione finora
- Surgery - Painless Scrotal SwellingDocumento23 pagineSurgery - Painless Scrotal Swellingismah_haron_1Nessuna valutazione finora
- Psy - Seminar Somato & PsychosomatoDocumento18 paginePsy - Seminar Somato & Psychosomatoismah_haron_1Nessuna valutazione finora
- Management of Upper Urinary Tract Obstruction: By: Siti Nurulismah BT Che HaronDocumento12 pagineManagement of Upper Urinary Tract Obstruction: By: Siti Nurulismah BT Che Haronismah_haron_1Nessuna valutazione finora
- Forensic Sudden DeathDocumento10 pagineForensic Sudden Deathismah_haron_1Nessuna valutazione finora
- ENT Case Bell's PalsyDocumento21 pagineENT Case Bell's Palsyismah_haron_1Nessuna valutazione finora
- Ortho - Conus Medullaris and Cauda Equina SyndromeDocumento16 pagineOrtho - Conus Medullaris and Cauda Equina Syndromeismah_haron_1100% (1)
- Chronic Complications: By: Siti Nurulismah BT Che HaronDocumento16 pagineChronic Complications: By: Siti Nurulismah BT Che Haronismah_haron_1Nessuna valutazione finora
- Medicine - Ix & TX HFDocumento19 pagineMedicine - Ix & TX HFismah_haron_1Nessuna valutazione finora
- Surgery Y3 MynotesDocumento5 pagineSurgery Y3 Mynotesismah_haron_1Nessuna valutazione finora
- Surgical ScarsDocumento2 pagineSurgical Scarsismah_haron_1Nessuna valutazione finora
- Surgery - Umbilical and Hypogastrium PainDocumento23 pagineSurgery - Umbilical and Hypogastrium Painismah_haron_1Nessuna valutazione finora
- A&E IntroSHOCKDocumento10 pagineA&E IntroSHOCKismah_haron_1Nessuna valutazione finora
- Paeds Y3 NotesDocumento5 paginePaeds Y3 Notesismah_haron_1Nessuna valutazione finora
- Paeds Seminar (Dengue Infection)Documento44 paginePaeds Seminar (Dengue Infection)ismah_haron_1Nessuna valutazione finora
- O&G - Perinatal Mortality IntroDocumento13 pagineO&G - Perinatal Mortality Introismah_haron_1Nessuna valutazione finora
- O&g Yr3 NotesDocumento4 pagineO&g Yr3 Notesismah_haron_1Nessuna valutazione finora
- Medicine Yr3 NotesDocumento3 pagineMedicine Yr3 Notesismah_haron_1Nessuna valutazione finora
- O&g - Case - Pih, PPDocumento19 pagineO&g - Case - Pih, PPismah_haron_1Nessuna valutazione finora
- Periodontal Disease May Increase Risk of Oral CancerDocumento8 paginePeriodontal Disease May Increase Risk of Oral Cancerمحمد العراقيNessuna valutazione finora
- We Are What... What We EatDocumento17 pagineWe Are What... What We EatАнастасия Пинькевич100% (1)
- Science 4 1st Summative TestDocumento2 pagineScience 4 1st Summative TestEmz FloresNessuna valutazione finora
- Emergency Medical Technician CPGs PDFDocumento121 pagineEmergency Medical Technician CPGs PDFAnonymous OdW7ev100% (1)
- A5 Pig Management GuidlinesDocumento4 pagineA5 Pig Management GuidlinesAnna NdunaNessuna valutazione finora
- Pediatric Cardiac Patients: History TakingDocumento31 paginePediatric Cardiac Patients: History TakingnovylatifahNessuna valutazione finora
- Renr Practice Test 9 FinalDocumento12 pagineRenr Practice Test 9 FinalTk100% (2)
- PLE 2019 - Medicine Questions and Answer KeyDocumento24 paginePLE 2019 - Medicine Questions and Answer KeydicksonNessuna valutazione finora
- Heat Illness Types, Causes, Symptoms and TreatmentsDocumento46 pagineHeat Illness Types, Causes, Symptoms and TreatmentsDewi Pertiwi Pertiwi0% (1)
- Kala-Azar (Leishmaniasis) Symptoms, Signs, DiagnosisDocumento36 pagineKala-Azar (Leishmaniasis) Symptoms, Signs, Diagnosisatulbd2006Nessuna valutazione finora
- Zinc Oxide-Eugenol and Calcium HydroxideDocumento5 pagineZinc Oxide-Eugenol and Calcium HydroxideJulioNessuna valutazione finora
- Problem SetDocumento2 pagineProblem Sethlc34Nessuna valutazione finora
- Enterobacter QuizDocumento8 pagineEnterobacter QuizDan Paolo Sanchez100% (2)
- Efects of Inspiratory Muscle Training in Older AdultsDocumento10 pagineEfects of Inspiratory Muscle Training in Older AdultsMaría Camila Zuluaga AriasNessuna valutazione finora
- Management of Infants BornDocumento6 pagineManagement of Infants BornDiana FlorezNessuna valutazione finora
- 2019 International Symposium on Pediatric Audiology ScheduleDocumento3 pagine2019 International Symposium on Pediatric Audiology ScheduleEulalia JuanNessuna valutazione finora
- Treating Constipation and Anal Stenosis in a 7-Month-OldDocumento35 pagineTreating Constipation and Anal Stenosis in a 7-Month-OldAbigail CruzNessuna valutazione finora
- Managing Benign Breast ConditionsDocumento20 pagineManaging Benign Breast Conditionschristel chadidNessuna valutazione finora
- Review 02Documento2 pagineReview 02Vicki KimNessuna valutazione finora
- Steroid Tapering and Supportive Treatment Guidance V1.0 PDFDocumento1 paginaSteroid Tapering and Supportive Treatment Guidance V1.0 PDFNthutagaol TrusNessuna valutazione finora
- History and P.E. of The Integumentary SystemDocumento6 pagineHistory and P.E. of The Integumentary SystempazucenaNessuna valutazione finora
- Management of Upper Airway DisorderDocumento46 pagineManagement of Upper Airway DisorderSahana Rangarajan100% (1)
- Schizophrenia - Practice Essentials, Background, PathophysiologyDocumento10 pagineSchizophrenia - Practice Essentials, Background, PathophysiologydilaNessuna valutazione finora
- USMLE Images For The BoardsDocumento297 pagineUSMLE Images For The BoardsMulham Etki100% (3)
- Artificial MethodsDocumento23 pagineArtificial MethodsJanna Broqueza RodriguezNessuna valutazione finora
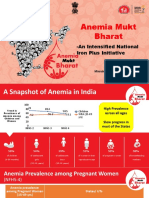
- Anemia Mukt Bharat: - An Intensified National Iron Plus InitiativeDocumento23 pagineAnemia Mukt Bharat: - An Intensified National Iron Plus InitiativeAnggun100% (1)
- Peyronies DiseaseDocumento6 paginePeyronies Diseaseapi-255601700Nessuna valutazione finora
- Nursing Care Plan: Change in Health Status As Evidence by Excessive Shaking After 1hour, The Patient Will Be Able ToDocumento1 paginaNursing Care Plan: Change in Health Status As Evidence by Excessive Shaking After 1hour, The Patient Will Be Able ToVoid LessNessuna valutazione finora
- Cardiovascular DisorderDocumento6 pagineCardiovascular DisorderClara De GuzmanNessuna valutazione finora
- Article 2 - NZMJ Midface FracturesDocumento9 pagineArticle 2 - NZMJ Midface FracturesIndra D KristionoNessuna valutazione finora