Potrebbero piacerti anche
- NeuroradiologyDocumento25 pagineNeuroradiologysarguss14100% (2)
- Small BowelDocumento4 pagineSmall Bowelsarguss14100% (1)
- From Doc Bandong's Own Words:: Shar 1 of 20Documento20 pagineFrom Doc Bandong's Own Words:: Shar 1 of 20sarguss14100% (1)
- Epidural and Spinal AnesthesiaDocumento86 pagineEpidural and Spinal Anesthesiasarguss1471% (7)
- NeuroradiologyDocumento11 pagineNeuroradiologysarguss14100% (2)
- Cardiac ImagingDocumento7 pagineCardiac Imagingsarguss14Nessuna valutazione finora
- Pleura and MediastinumDocumento16 paginePleura and Mediastinumsarguss14100% (1)
- Introduction To RadiologyDocumento3 pagineIntroduction To Radiologysarguss14Nessuna valutazione finora
- Thinking Outside The Box Creative Teaching MethodsDocumento83 pagineThinking Outside The Box Creative Teaching Methodsemmegi62Nessuna valutazione finora
- Pediatric GI RadiologyDocumento6 paginePediatric GI Radiologysarguss14Nessuna valutazione finora
- Management of The Sick Young Infant Age 1 Week Up To 2 MonthsDocumento5 pagineManagement of The Sick Young Infant Age 1 Week Up To 2 Monthsapi-19824701Nessuna valutazione finora
- IMMUNIZATION TIPSDocumento14 pagineIMMUNIZATION TIPSETCNessuna valutazione finora
- English File 4th Ed - Intermediate Plus - Student's BookDocumento170 pagineEnglish File 4th Ed - Intermediate Plus - Student's BookClara RoutaboulNessuna valutazione finora
- Neonatal Respiratory Distress Syndrome (RDS) Causes, Symptoms & TreatmentDocumento11 pagineNeonatal Respiratory Distress Syndrome (RDS) Causes, Symptoms & TreatmentHina MasoodNessuna valutazione finora
- Cyanotic Congenital Heart Diseases, Etc.Documento12 pagineCyanotic Congenital Heart Diseases, Etc.sarguss14100% (2)
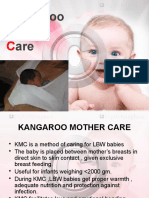
- Kangaroo Mother CareDocumento21 pagineKangaroo Mother CareM Fathur Arief KurniawanNessuna valutazione finora
- Ready For PET Teacher's BookDocumento66 pagineReady For PET Teacher's Bookalicia100% (1)
- Genitourinary SystemDocumento8 pagineGenitourinary Systemsarguss14100% (1)
- Notes On Baby Bath - Care of The Mother During The Postpartum PeriodDocumento12 pagineNotes On Baby Bath - Care of The Mother During The Postpartum PeriodOink TopusNessuna valutazione finora
- Nursing Care of At-Risk NewbornsDocumento256 pagineNursing Care of At-Risk NewbornsAaron ConstantinoNessuna valutazione finora
- Health Edu. On Breast Feedind WASEEM-1Documento7 pagineHealth Edu. On Breast Feedind WASEEM-1MysaraNessuna valutazione finora
- IMCI exercises assess sick young infantsDocumento2 pagineIMCI exercises assess sick young infantsJarzhieRhojeenNessuna valutazione finora
- High Risk New BornDocumento12 pagineHigh Risk New BornM. jehovah Nissie YeshalomeNessuna valutazione finora
- Anorectal Malformations: Presented by Khushveer KaurDocumento91 pagineAnorectal Malformations: Presented by Khushveer KaurKataria DavinNessuna valutazione finora
- Minor Disorders of Newborn and Nursing CareDocumento47 pagineMinor Disorders of Newborn and Nursing CarePOORNIMA B SNessuna valutazione finora
- Stage 1: Dorsal Induction: Pediatric NeuroradiologyDocumento8 pagineStage 1: Dorsal Induction: Pediatric Neuroradiologysarguss14100% (1)
- Expanding Knowledge of Caregiving EnvironmentsDocumento8 pagineExpanding Knowledge of Caregiving EnvironmentsMilagros FloritaNessuna valutazione finora
- Newborn CareDocumento49 pagineNewborn CareJohn Mark PocsidioNessuna valutazione finora
- Teaching Profession Review (Drill 1)Documento15 pagineTeaching Profession Review (Drill 1)Nico John Bauzon CapuaNessuna valutazione finora
- I. Acute Convulsions:: CNS Tonsillitis Otitis MediaDocumento2 pagineI. Acute Convulsions:: CNS Tonsillitis Otitis MediaJinky MonteagudoNessuna valutazione finora
- Inhalational Anesthetics: Patigas, Requinta, ResuelloDocumento88 pagineInhalational Anesthetics: Patigas, Requinta, Resuellosarguss140% (1)
- Ed-Child Febrile FitDocumento2 pagineEd-Child Febrile Fitmanish708345Nessuna valutazione finora
- Gallbladder, Liver, Pancreas and SpleenDocumento19 pagineGallbladder, Liver, Pancreas and Spleensarguss14100% (3)
- Pelvic Inflammatory DiseaseDocumento18 paginePelvic Inflammatory DiseaseVictorNessuna valutazione finora
- Treating Pneumonia in Children Under 5Documento38 pagineTreating Pneumonia in Children Under 5Arjumand AliNessuna valutazione finora
- Management of Breast FeedingDocumento17 pagineManagement of Breast FeedingUday KumarNessuna valutazione finora
- Febrile convulsions: assessment, treatment and educationDocumento12 pagineFebrile convulsions: assessment, treatment and educationPalash NagdeoteNessuna valutazione finora
- Rationale For An Integrated Approach in The Management of Sick ChildrenDocumento42 pagineRationale For An Integrated Approach in The Management of Sick ChildrenRIK HAROLD GATPANDANNessuna valutazione finora
- Case Report "Febrile Seizures": Betsheba E. S. 123307018Documento37 pagineCase Report "Febrile Seizures": Betsheba E. S. 123307018AmandaRizkaNessuna valutazione finora
- MANAGING SICK CHILDREN AGES 2 MONTHS TO 5 YEARSDocumento6 pagineMANAGING SICK CHILDREN AGES 2 MONTHS TO 5 YEARSChristian PoroyNessuna valutazione finora
- Minordisordersofbnewborn 161129154708Documento33 pagineMinordisordersofbnewborn 161129154708Kevin Daniel GoveasNessuna valutazione finora
- INTRODUCTIONDocumento26 pagineINTRODUCTIONTina Manoj100% (1)
- Pellagra: Elaborated By:tambur Vadim Group:M2016Documento11 paginePellagra: Elaborated By:tambur Vadim Group:M2016vadim tamburNessuna valutazione finora
- 03.chronic Supp Otitis MediaDocumento33 pagine03.chronic Supp Otitis MediaJumanne JayNessuna valutazione finora
- Preterm Labour and Preterm Rupture of Membranes: by Prof - Farouk Abdel AzizDocumento23 paginePreterm Labour and Preterm Rupture of Membranes: by Prof - Farouk Abdel AziznasibdinNessuna valutazione finora
- Understanding Diarrhea: Causes, Symptoms, Prevention and ManagementDocumento12 pagineUnderstanding Diarrhea: Causes, Symptoms, Prevention and ManagementSoumya RajeswariNessuna valutazione finora
- Review of Systems Checklist for Pediatric Physical ExamDocumento2 pagineReview of Systems Checklist for Pediatric Physical ExamteuuuuNessuna valutazione finora
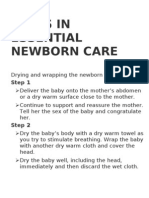
- Steps in Essential Newborn CareDocumento12 pagineSteps in Essential Newborn CareCedy L. CieloNessuna valutazione finora
- National Policy For ChildrenDocumento5 pagineNational Policy For Childrenthilaga88Nessuna valutazione finora
- MANAGEMENT OF THE SICK CHILDDocumento6 pagineMANAGEMENT OF THE SICK CHILDclarNessuna valutazione finora
- PrematurityDocumento37 paginePrematurityNishaThakuriNessuna valutazione finora
- Hypothermia in Neonates PresentationDocumento18 pagineHypothermia in Neonates PresentationIshNessuna valutazione finora
- Neonatal Jaundice Guide: Causes, Symptoms, DiagnosisDocumento3 pagineNeonatal Jaundice Guide: Causes, Symptoms, DiagnosismeidyNessuna valutazione finora
- Febrile Convulsions in ChildrenDocumento2 pagineFebrile Convulsions in ChildrenMagdalena Dwiyani HutajuluNessuna valutazione finora
- Newborn Resuscitation GuidelinesDocumento7 pagineNewborn Resuscitation GuidelinesYwagar YwagarNessuna valutazione finora
- Patient InformationDocumento15 paginePatient InformationPriyanjali SainiNessuna valutazione finora
- Nursing Care of A Neonate Part 1Documento67 pagineNursing Care of A Neonate Part 1Rani G SNessuna valutazione finora
- A Study To Assess The Effectiveness of Structured Teaching Programme On Knowledge Regarding Management of Low Birth Weight LBW Babies Among Postnatal Mothers in Selected Community at GwaliorDocumento7 pagineA Study To Assess The Effectiveness of Structured Teaching Programme On Knowledge Regarding Management of Low Birth Weight LBW Babies Among Postnatal Mothers in Selected Community at GwaliorEditor IJTSRDNessuna valutazione finora
- Immediate Newborn Care (Autosaved)Documento183 pagineImmediate Newborn Care (Autosaved)mftaganasNessuna valutazione finora
- Essential Newborn CareDocumento20 pagineEssential Newborn Carejanjan_cepilloNessuna valutazione finora
- Postmature Infants 1Documento13 paginePostmature Infants 1LyssaMarieKathryneEge100% (1)
- Respiratory Distress Syndrome: Islamic University Nursing CollegeDocumento21 pagineRespiratory Distress Syndrome: Islamic University Nursing Collegeyaumil agisnaNessuna valutazione finora
- 6-Health Problems Common in PreschoolerDocumento36 pagine6-Health Problems Common in PreschoolerPam Lala100% (2)
- Management of Neonatal HypoglycemiaDocumento14 pagineManagement of Neonatal Hypoglycemiaece142Nessuna valutazione finora
- Therapeutic PlayDocumento9 pagineTherapeutic PlayVivek PrabhakarNessuna valutazione finora
- Febrile Seizure Case FileDocumento4 pagineFebrile Seizure Case Filehttps://medical-phd.blogspot.comNessuna valutazione finora
- Nicu ReportDocumento66 pagineNicu ReportEr Shah Rukh QadriNessuna valutazione finora
- Nutrition Essentials for Growing PreschoolersDocumento6 pagineNutrition Essentials for Growing PreschoolersKeerthana VNessuna valutazione finora
- Abnormal Amniotic Fluid LevelsDocumento29 pagineAbnormal Amniotic Fluid LevelsSTAR Plus SerialsNessuna valutazione finora
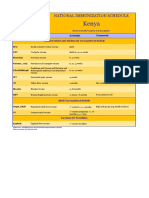
- Kenya Immunization ScheduleDocumento1 paginaKenya Immunization ScheduleDani AnyikaNessuna valutazione finora
- Episiotomy Wound Haematoma: Recognition, Management and Healing Assessment by REEDA Scale in Postpartum PeriodDocumento4 pagineEpisiotomy Wound Haematoma: Recognition, Management and Healing Assessment by REEDA Scale in Postpartum PeriodIOSRjournalNessuna valutazione finora
- Nursing Pediatric Case StudyDocumento9 pagineNursing Pediatric Case StudyKJay Solijon100% (1)
- Homemade Oatmeal Bath Relieves Chickenpox ItchDocumento7 pagineHomemade Oatmeal Bath Relieves Chickenpox ItchShahzada KhurramNessuna valutazione finora
- Infants Diabetic MothersDocumento17 pagineInfants Diabetic MothersJaya PrabhaNessuna valutazione finora
- Extremely Low Birth Weight (ELBW) InfantDocumento48 pagineExtremely Low Birth Weight (ELBW) InfanthannanyusofNessuna valutazione finora
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesDa EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNessuna valutazione finora
- Preoperative EvaluationDocumento25 paginePreoperative Evaluationsarguss14Nessuna valutazione finora
- World Gastroenterology Organization Global GuidelineDocumento29 pagineWorld Gastroenterology Organization Global GuidelineRizky Rachmania AmandaNessuna valutazione finora
- Axial Arthritis: Degenerative Annular DiseaseDocumento18 pagineAxial Arthritis: Degenerative Annular Diseasesarguss14100% (1)
- Male PelvisDocumento8 pagineMale Pelvissarguss14100% (1)
- Male Genital TractDocumento7 pagineMale Genital Tractsarguss14Nessuna valutazione finora
- Kidney, Ureter, BladderDocumento12 pagineKidney, Ureter, Bladdersarguss14100% (1)
- Genitourinary SystemDocumento8 pagineGenitourinary Systemsarguss14100% (1)
- Introduction To RadiologyDocumento3 pagineIntroduction To Radiologysarguss14Nessuna valutazione finora
- CNS Tumors and Infections Part1Documento2 pagineCNS Tumors and Infections Part1sarguss14100% (1)
- CNS Tumors and Infections Part3Documento6 pagineCNS Tumors and Infections Part3sarguss14100% (1)
- Extracerebral Hemorrhage, Etc.Documento14 pagineExtracerebral Hemorrhage, Etc.sarguss14Nessuna valutazione finora
- ArthritisDocumento9 pagineArthritissarguss14100% (1)
- Congenital Cystic Adenomatoid Malformation (CCAM)Documento7 pagineCongenital Cystic Adenomatoid Malformation (CCAM)sarguss14Nessuna valutazione finora
- CNS Tumors and Infections Part2Documento2 pagineCNS Tumors and Infections Part2sarguss14Nessuna valutazione finora
- Chest RadiologyDocumento3 pagineChest Radiologysarguss14Nessuna valutazione finora
- Bone TumorsDocumento15 pagineBone Tumorssarguss1450% (2)
- LearnEnglish Audio Zone Learning LanguagesDocumento4 pagineLearnEnglish Audio Zone Learning LanguagesrominaNessuna valutazione finora
- District Monitoring Evaluation AdjustmentDocumento21 pagineDistrict Monitoring Evaluation AdjustmentReycel Miravalles TolentinoNessuna valutazione finora
- Cambridge International AS & A Level: English LanguageDocumento15 pagineCambridge International AS & A Level: English Languagejbcoker05Nessuna valutazione finora
- Lab 05: Joining Tables: JoinsDocumento4 pagineLab 05: Joining Tables: JoinsNida FiazNessuna valutazione finora
- Dalits in India Sagarika Ghosh sOCIAL rESEARCH 2003Documento28 pagineDalits in India Sagarika Ghosh sOCIAL rESEARCH 2003ghisaram100% (1)
- Nguyen Lucie Field Experience Log PleDocumento7 pagineNguyen Lucie Field Experience Log Pleapi-590751914Nessuna valutazione finora
- Statement of Purpose (SOP)Documento2 pagineStatement of Purpose (SOP)Subha Sharma PoudelNessuna valutazione finora
- College Essay Rubric 2013Documento2 pagineCollege Essay Rubric 2013Nicholas Crothers100% (2)
- Game SenseDocumento6 pagineGame Senseapi-408301186Nessuna valutazione finora
- MCE DatasheetDocumento2 pagineMCE DatasheetH Awad MahgoubNessuna valutazione finora
- Ready or Not - How Do We Accelerate The Developmental Readiness of Leaders PDFDocumento7 pagineReady or Not - How Do We Accelerate The Developmental Readiness of Leaders PDFCarol MagriNessuna valutazione finora
- Classroom ArrangementsDocumento5 pagineClassroom Arrangementsapi-427868008Nessuna valutazione finora
- Assignment II: More Memorize: ObjectiveDocumento7 pagineAssignment II: More Memorize: ObjectiveAlbert JordanNessuna valutazione finora
- This Lesson PDF - 7.2.3 - Internal Auditor CompetencyDocumento10 pagineThis Lesson PDF - 7.2.3 - Internal Auditor CompetencyThee BouyyNessuna valutazione finora
- Client Alert: Moore Sparks, LLCDocumento1 paginaClient Alert: Moore Sparks, LLCWanda HarrisNessuna valutazione finora
- Vygotsky Theory DoneDocumento4 pagineVygotsky Theory DoneLubaba ShabbirNessuna valutazione finora
- Alt Wellness Syllabus Fa102Documento30 pagineAlt Wellness Syllabus Fa102Shar MurphyNessuna valutazione finora
- Activity No.3-Problems and Obstacles To Economic Growth in Less Developed Countries-LOPEZ, JOEBIN C.Documento1 paginaActivity No.3-Problems and Obstacles To Economic Growth in Less Developed Countries-LOPEZ, JOEBIN C.Joebin Corporal LopezNessuna valutazione finora
- Jurnal Gizi Prima JGP (TGS)Documento6 pagineJurnal Gizi Prima JGP (TGS)dikaNessuna valutazione finora
- DLL Tle He 6 Q1 W5Documento5 pagineDLL Tle He 6 Q1 W5Louie EscuderoNessuna valutazione finora
- Associate Pianist The Royal Ballet JDApr 22Documento2 pagineAssociate Pianist The Royal Ballet JDApr 22SaraNessuna valutazione finora
- Guidance & CounselingDocumento6 pagineGuidance & CounselingTaimoor KhanNessuna valutazione finora
- Cybrary SOC Analyst Level 1 Syllabus 1Documento10 pagineCybrary SOC Analyst Level 1 Syllabus 1Mohana DatlaNessuna valutazione finora
- Department of Education: Republic of The PhilppinesDocumento21 pagineDepartment of Education: Republic of The PhilppinesshairaNessuna valutazione finora
- Budget of Work - Creative WritingDocumento1 paginaBudget of Work - Creative WritingNeil VillasNessuna valutazione finora
- Interview of A Tourism ExpertDocumento2 pagineInterview of A Tourism ExpertDianna Kyla Cabacis UyNessuna valutazione finora