Potrebbero piacerti anche
- Stephen C. Wood, Ph.D. Medical Physiology Metabolic Rate and Alveolar VentilationDocumento9 pagineStephen C. Wood, Ph.D. Medical Physiology Metabolic Rate and Alveolar VentilationSimran SukhijaNessuna valutazione finora
- Case StudiesDocumento4 pagineCase StudiesSimran SukhijaNessuna valutazione finora
- C2 VertebraDocumento4 pagineC2 VertebraSimran SukhijaNessuna valutazione finora
- C2 VertebraDocumento4 pagineC2 VertebraSimran SukhijaNessuna valutazione finora
- C2 VertebraDocumento4 pagineC2 VertebraSimran SukhijaNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Preoperative NICE GuidelinesDocumento117 paginePreoperative NICE GuidelinesDana ApelaNessuna valutazione finora
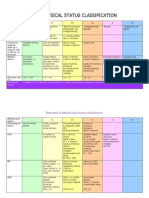
- Asa Physical Status Classification SystemDocumento2 pagineAsa Physical Status Classification SystemWanditoGayuhUtomoNessuna valutazione finora
- ASA Physical Status ClassificationDocumento1 paginaASA Physical Status ClassificationАндрій ДанильцівNessuna valutazione finora
- (Surg2) 5.1a Introduction To Anesthesia Part 1Documento21 pagine(Surg2) 5.1a Introduction To Anesthesia Part 1AlloiBialbaNessuna valutazione finora
- Postoperative Infection and Mortality Following Elective Surgery in The International Surgical Outcomes Study (ISOS)Documento32 paginePostoperative Infection and Mortality Following Elective Surgery in The International Surgical Outcomes Study (ISOS)Antonio Carlos Betanzos PlanellNessuna valutazione finora
- ASA Physical Status Classification System - UpToDateDocumento2 pagineASA Physical Status Classification System - UpToDateDaniel Rico FuentesNessuna valutazione finora
- Asa Physical Status Classification System - Asa House of Delegates On October 15, 2014 - Asa-PhysicalDocumento2 pagineAsa Physical Status Classification System - Asa House of Delegates On October 15, 2014 - Asa-PhysicalLourdes100% (1)
- Rapid Geriatric Assessment of Hip FractureDocumento14 pagineRapid Geriatric Assessment of Hip FractureJuliana Moreno LadinoNessuna valutazione finora
- Pharmacological Behavior ManagementDocumento45 paginePharmacological Behavior Managementdeepesh jaiswalNessuna valutazione finora
- Anaesthetic Case StudyDocumento11 pagineAnaesthetic Case StudysomyntNessuna valutazione finora
- Spinal Surgery in Patients Aged 80 Years and Older: Risk Stratification Using The Modified Frailty IndexDocumento8 pagineSpinal Surgery in Patients Aged 80 Years and Older: Risk Stratification Using The Modified Frailty IndexMuhammad DzulfikarNessuna valutazione finora
- بسم هللا الرحمن الرحيم Surgical Site Infection PreventionDocumento98 pagineبسم هللا الرحمن الرحيم Surgical Site Infection PreventionHosam GomaaNessuna valutazione finora
- Special Care in DentistryDocumento508 pagineSpecial Care in DentistryMaha MeftahNessuna valutazione finora
- ASA Physical Status Classification System 2019Documento2 pagineASA Physical Status Classification System 2019hquinarNessuna valutazione finora
- ASA physical status classification guideDocumento3 pagineASA physical status classification guideMelisa Malik0% (1)
- Asa Physical Status Classification SystemDocumento2 pagineAsa Physical Status Classification SystemPandhu SuproboNessuna valutazione finora
- Asa 2013Documento1.076 pagineAsa 2013Marwa Mahrous100% (4)
- ASA Physical Status Classification System GuideDocumento2 pagineASA Physical Status Classification System Guidejackie funtanillaNessuna valutazione finora
- Asa ClassDocumento3 pagineAsa ClassPriska Gusti Wulandari67% (3)
- US - ASA Physical Status Classification Chart - V2Documento1 paginaUS - ASA Physical Status Classification Chart - V2Roberto PvetNessuna valutazione finora
- Munro Pressure Ulcer Risk Assessment ScaleDocumento5 pagineMunro Pressure Ulcer Risk Assessment ScaleIkar Swito100% (1)
- Essential Preop AssessmentDocumento41 pagineEssential Preop AssessmentTan Chuan HsinNessuna valutazione finora
- 1 Guidelines For Anesthetic Management in Clinical PracticeDocumento54 pagine1 Guidelines For Anesthetic Management in Clinical PracticeAMVAC RomaniaNessuna valutazione finora
- ASA Physical Status Classification SystemDocumento2 pagineASA Physical Status Classification SystemNadya Kaulika ListyaniNessuna valutazione finora
- Moderate Sedation PowerpointDocumento68 pagineModerate Sedation PowerpointJames GarnerNessuna valutazione finora
- Preoperative Anesthesia and PremedicationDocumento25 paginePreoperative Anesthesia and Premedicationnadya fachfudyanaNessuna valutazione finora
- Preoperative AssessmentDocumento41 paginePreoperative Assessmentansuh22100% (1)
- ASA Physical Status Classification System PDFDocumento6 pagineASA Physical Status Classification System PDFfbihansipNessuna valutazione finora
- American Society of Anesthesiologists Classification (ASA Class) - StatPearls - NCBI BookshelfDocumento3 pagineAmerican Society of Anesthesiologists Classification (ASA Class) - StatPearls - NCBI BookshelfErikaMRSiaNessuna valutazione finora
- ASA Classification PDFDocumento2 pagineASA Classification PDFgodfather_exeNessuna valutazione finora