Potrebbero piacerti anche
- Soluble Liver Antigen/liver-Pancreas Antigen (anti-SLA/LP) AntibodiesDocumento11 pagineSoluble Liver Antigen/liver-Pancreas Antigen (anti-SLA/LP) AntibodiesShiela Montances100% (1)
- Chapter 8Documento89 pagineChapter 8Harith AtrisNessuna valutazione finora
- Lectu RioDocumento7 pagineLectu RioTselmeg TselmegNessuna valutazione finora
- Non Viral HepatitisDocumento40 pagineNon Viral Hepatitisostaz2000100% (1)
- Peptic Ulcers - Cirrhosis - Alcoholic Liver DiseaseDocumento5 paginePeptic Ulcers - Cirrhosis - Alcoholic Liver DiseaseShubhamNessuna valutazione finora
- Clinical Chemistry LiverDocumento6 pagineClinical Chemistry LiverMustafa Salah MahdiNessuna valutazione finora
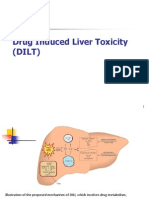
- Drug Induced Liver Toxicity-FinalDocumento39 pagineDrug Induced Liver Toxicity-FinalAjeng SekariniNessuna valutazione finora
- Hepatobiliary CasesDocumento55 pagineHepatobiliary CasesMeghana MaddaliNessuna valutazione finora
- Chronic Liver Disease and CirrhosisDocumento5 pagineChronic Liver Disease and Cirrhosisaqil ithninNessuna valutazione finora
- Fiziopatologie (English (British) )Documento22 pagineFiziopatologie (English (British) )Alina VoineaNessuna valutazione finora
- Drug Induced Liver DiseaseDocumento15 pagineDrug Induced Liver DiseaseMUGHALNessuna valutazione finora
- Chronic Liver FailureDocumento4 pagineChronic Liver FailureJasmine Faith SilvaNessuna valutazione finora
- Unit 4 - Acute Liver FailureDocumento5 pagineUnit 4 - Acute Liver FailureMa. Felice CristobalNessuna valutazione finora
- Clinical Pharmacokinetics in Liver Failure Patients SenddDocumento30 pagineClinical Pharmacokinetics in Liver Failure Patients Senddthavia andrianiNessuna valutazione finora
- Drug Induced Liver Toxicity (DILD)Documento39 pagineDrug Induced Liver Toxicity (DILD)Surya Pratama100% (1)
- Anaesthesia For Patients With Liver DiseaseDocumento5 pagineAnaesthesia For Patients With Liver DiseaseRitu BhandariNessuna valutazione finora
- Fulminant Hepatic FailureDocumento10 pagineFulminant Hepatic FailureAira Anne Tonee VillaminNessuna valutazione finora
- HepatitisDocumento4 pagineHepatitisAlambusha ShuklaNessuna valutazione finora
- Hepatic EncephalopathyDocumento5 pagineHepatic Encephalopathyliveconnectionz282Nessuna valutazione finora
- Panagiota Myrto Dramitinou F.N. 7915 Group 61: Questions Related To Hepatitis ADocumento3 paginePanagiota Myrto Dramitinou F.N. 7915 Group 61: Questions Related To Hepatitis AΜυρτώ ΔραμητινούNessuna valutazione finora
- Cirrhosis: Author: David C Wolf, MD, FACP, FACG, AGAF, Medical Director of LiverDocumento29 pagineCirrhosis: Author: David C Wolf, MD, FACP, FACG, AGAF, Medical Director of LiverdahsyatnyaNessuna valutazione finora
- Diagnosis and Treatment of Liver DiseaseDocumento5 pagineDiagnosis and Treatment of Liver DiseaseHéctor MaldonadoNessuna valutazione finora
- Pathophysiology - LiverDocumento3 paginePathophysiology - LiverΜυρτώ ΔραμητινούNessuna valutazione finora
- Drug Induced Hepatitis: Dr.M.Sharmila Assistant Professor M7 (Prof CR Unit) Institute of Internal MedicineDocumento21 pagineDrug Induced Hepatitis: Dr.M.Sharmila Assistant Professor M7 (Prof CR Unit) Institute of Internal MedicineAtakan Yeşil100% (1)
- Pharmacotherapy of Hepatic FailureDocumento11 paginePharmacotherapy of Hepatic FailureMenna ElesawyNessuna valutazione finora
- College of Medicine: Thi Qar UniversityDocumento30 pagineCollege of Medicine: Thi Qar Universityhussain AltaherNessuna valutazione finora
- Atlas of Liver Pathology - Chapter 8 Biliary Tree DiseaseDocumento45 pagineAtlas of Liver Pathology - Chapter 8 Biliary Tree DiseaseShabir HussainNessuna valutazione finora
- Liver TransplantationDocumento21 pagineLiver TransplantationRozi RamliNessuna valutazione finora
- Alcoholic Liver Disease: Last Updated: January 19, 2024Documento16 pagineAlcoholic Liver Disease: Last Updated: January 19, 2024Tselmeg TselmegNessuna valutazione finora
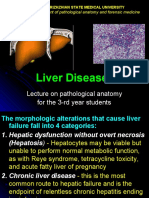
- Liver Diseases: Lecture On Pathological Anatomy For The 3-rd Year StudentsDocumento27 pagineLiver Diseases: Lecture On Pathological Anatomy For The 3-rd Year StudentsRodriguez Vivanco Kevin DanielNessuna valutazione finora
- PR03671Documento4 paginePR03671Dalia ExtrapolisNessuna valutazione finora
- Sirrhosis HatiDocumento6 pagineSirrhosis HatikimokberusungNessuna valutazione finora
- Dr. S.P. Hewawasam (MD) Consultant Gastroenterologist/Senior Lecturer in PhysiologyDocumento33 pagineDr. S.P. Hewawasam (MD) Consultant Gastroenterologist/Senior Lecturer in PhysiologyAjung SatriadiNessuna valutazione finora
- Acute Liver FailureDocumento7 pagineAcute Liver FailureIbrahim RegachoNessuna valutazione finora
- Cirrosis HepaticaDocumento10 pagineCirrosis Hepaticaadriel710Nessuna valutazione finora
- Hepatic Encephalopathy: Causes, Tests, and Treatment OptionsDa EverandHepatic Encephalopathy: Causes, Tests, and Treatment OptionsValutazione: 3.5 su 5 stelle3.5/5 (2)
- Cirrhosis of LiverDocumento6 pagineCirrhosis of LiverpakdejackNessuna valutazione finora
- Hepatological Diseases in AnimalsDocumento34 pagineHepatological Diseases in AnimalsRICHARD RODERICK OLMEDONessuna valutazione finora
- Nonalcoholic Fatty Liver - StatPearls - NCBI Bookshelf PDFDocumento6 pagineNonalcoholic Fatty Liver - StatPearls - NCBI Bookshelf PDFMr BrewokNessuna valutazione finora
- Acute Liver FailureDocumento3 pagineAcute Liver FailureElisabeth F. OjhaNessuna valutazione finora
- Cirrosis Adnd Its ComplicationDocumento50 pagineCirrosis Adnd Its Complicationnathan asfahaNessuna valutazione finora
- Cholestatic DiseasesDocumento12 pagineCholestatic DiseasesJohNessuna valutazione finora
- 6 Kuliah Liver CirrhosisDocumento55 pagine6 Kuliah Liver CirrhosisAnonymous vUEDx8100% (1)
- Alcoholic Liver Disease - StatPearls - NCBI BookshelfDocumento10 pagineAlcoholic Liver Disease - StatPearls - NCBI Bookshelfd99452727Nessuna valutazione finora
- Falla Hepatica GastroDocumento12 pagineFalla Hepatica GastrolouispekasNessuna valutazione finora
- Anesthesiaforliver Transplantation: Dieter Adelmann,, Kate Kronish,, Michael A. RamsayDocumento18 pagineAnesthesiaforliver Transplantation: Dieter Adelmann,, Kate Kronish,, Michael A. RamsayJZNessuna valutazione finora
- Acute Glomerulonephritis: By: Jhaziel E. BermejoDocumento20 pagineAcute Glomerulonephritis: By: Jhaziel E. BermejoJhaziel BermejoNessuna valutazione finora
- Molecular Toxicology 2Documento67 pagineMolecular Toxicology 2Tira MaharaniNessuna valutazione finora
- CirrosisDocumento44 pagineCirrosisflorilett marian cifuentesNessuna valutazione finora
- ATT Induced Hepatotoxicity: Dr. K. K. SharmaDocumento36 pagineATT Induced Hepatotoxicity: Dr. K. K. SharmaSucharita Ray100% (1)
- Assessment of Jaundice in The Hospitalized Patient PDFDocumento16 pagineAssessment of Jaundice in The Hospitalized Patient PDFlaura canoNessuna valutazione finora
- Acute Tubular NecrosisDocumento46 pagineAcute Tubular NecrosispadmaNessuna valutazione finora
- Acute PancreatitisDocumento25 pagineAcute PancreatitisSunil YadavNessuna valutazione finora
- Approach To The Jaundiced Cat - WSAVA 2015 Congress - VINDocumento6 pagineApproach To The Jaundiced Cat - WSAVA 2015 Congress - VINdmantsioNessuna valutazione finora
- Alcoholic Liver DiseaseDocumento26 pagineAlcoholic Liver DiseaseSaifNessuna valutazione finora
- Hepatitis: Classification and External ResourcesDocumento7 pagineHepatitis: Classification and External ResourcesWisnu AdiputraNessuna valutazione finora
- Liver Cirrhosis and Hepatocellular FailureDocumento36 pagineLiver Cirrhosis and Hepatocellular FailureLedia EssamNessuna valutazione finora
- Patho4-6 - Liver (Dr. Dy)Documento13 paginePatho4-6 - Liver (Dr. Dy)miguel cuevas100% (1)
- The Most Common Presenting Symptoms in CD Are Fatigue and Abdominal Pain While in UC Bloody BM and Diarrhea Are Most CommonDocumento3 pagineThe Most Common Presenting Symptoms in CD Are Fatigue and Abdominal Pain While in UC Bloody BM and Diarrhea Are Most CommonElle ReyesNessuna valutazione finora
- Module 3. Pathology of pregnancy, labor and puerperium: Test for topic 4 Огляд спроби 2Documento9 pagineModule 3. Pathology of pregnancy, labor and puerperium: Test for topic 4 Огляд спроби 2Sarfaraz ansariNessuna valutazione finora
- Venous Thromboembolism (VTE) Pathophysiology September 2016Documento46 pagineVenous Thromboembolism (VTE) Pathophysiology September 2016Nick GouvatsosNessuna valutazione finora
- Iris Anatomy MmeDocumento4 pagineIris Anatomy MmeSatyam ChaudharyNessuna valutazione finora
- The Heart As A PumpDocumento25 pagineThe Heart As A PumpBali PalNessuna valutazione finora
- Test Bank For Comprehensive Perinatal and Pediatric Respiratory Care 4th Edition by Whitaker Isbn 10 1439059438 Isbn 13 9781439059432Documento7 pagineTest Bank For Comprehensive Perinatal and Pediatric Respiratory Care 4th Edition by Whitaker Isbn 10 1439059438 Isbn 13 9781439059432trangdatif0Nessuna valutazione finora
- Manicure and Pedicure Services: NtroductionDocumento29 pagineManicure and Pedicure Services: Ntroductionanshuman singhNessuna valutazione finora
- The University of Chicago PressDocumento47 pagineThe University of Chicago PressNissa SissariNessuna valutazione finora
- Blood and Circulation PDFDocumento47 pagineBlood and Circulation PDFeric sivaneshNessuna valutazione finora
- Ectopic Pregnancy ImportantDocumento42 pagineEctopic Pregnancy Importantﻣﻠﻚ عيسىNessuna valutazione finora
- Hoeltke Chapter5 RevisedDocumento34 pagineHoeltke Chapter5 RevisedPrincess Weiyoung100% (1)
- ABO DiscrepanicesDocumento12 pagineABO DiscrepanicesGlenn PerezNessuna valutazione finora
- MCQ Blood Physiology SermadDocumento22 pagineMCQ Blood Physiology SermadAsif Hanif50% (4)
- National ECG Workshop AIMST MMA 2015Documento217 pagineNational ECG Workshop AIMST MMA 2015Sara100% (1)
- 1 - The Skin's Function PDFDocumento9 pagine1 - The Skin's Function PDFskoahNessuna valutazione finora
- Blood Circulation and TransportDocumento28 pagineBlood Circulation and TransportZam EjamNessuna valutazione finora
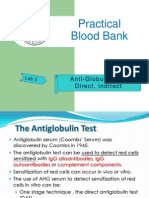
- Lab 5 Coombs TestsDocumento26 pagineLab 5 Coombs TestsJennifer DixonNessuna valutazione finora
- AssignmentLec2 DimnatangDocumento2 pagineAssignmentLec2 DimnatangFatimah DimnatangNessuna valutazione finora
- Fracture and Dislocation-Rahardyan Magetsari (2016) PDFDocumento105 pagineFracture and Dislocation-Rahardyan Magetsari (2016) PDFRobertOktaChandraNessuna valutazione finora
- 978-0321919007 Essentials of HumanDocumento11 pagine978-0321919007 Essentials of HumanRobinson1Nessuna valutazione finora
- Tips For Ust Med FreshmenDocumento3 pagineTips For Ust Med FreshmenFred EvidorNessuna valutazione finora
- Life ProcessesDocumento15 pagineLife ProcessesShalom LogosNessuna valutazione finora
- First Summative Test in SCIENCE 5 2nd QuarterDocumento2 pagineFirst Summative Test in SCIENCE 5 2nd QuarterGrace Cruz Delos Reyes89% (9)
- Material Mini NetterDocumento13 pagineMaterial Mini NetterVALENTINA ALBORNOZ BASTÍASNessuna valutazione finora
- Life ProcessesDocumento7 pagineLife Processesomkar108140% (1)
- OMM Study GuideDocumento53 pagineOMM Study Guideshadowcrest12100% (5)
- Sesi 6-Fisiologi Neuromuskuler IDocumento86 pagineSesi 6-Fisiologi Neuromuskuler IGiselleNessuna valutazione finora
- Grade 10 ReviewerDocumento55 pagineGrade 10 ReviewerwkwjwjbsdNessuna valutazione finora
- Cardiovascular PDFDocumento8 pagineCardiovascular PDFLyka AbajaNessuna valutazione finora
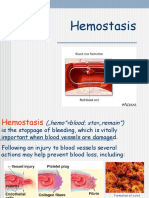
- Lecture HemostasisDocumento28 pagineLecture HemostasisЛариса ТкачеваNessuna valutazione finora
- Biomedical InstrumentationDocumento16 pagineBiomedical Instrumentationshaswatece100% (6)