Potrebbero piacerti anche
- Living with Concepts: Anthropology in the Grip of RealityDa EverandLiving with Concepts: Anthropology in the Grip of RealityAndrew BrandelNessuna valutazione finora
- Personal Research PhilosophyDocumento12 paginePersonal Research PhilosophyAndy MarsigliaNessuna valutazione finora
- Perspectives: Redemption, Economics, Law, Justice, Mediation, Human Rights: Redemption, Economics, Law, Justice, Mediation, Human RightsDa EverandPerspectives: Redemption, Economics, Law, Justice, Mediation, Human Rights: Redemption, Economics, Law, Justice, Mediation, Human RightsNessuna valutazione finora
- Book of AbstractsDocumento60 pagineBook of AbstractsANDREASNessuna valutazione finora
- Collective Wisdom in the West: Beyond the shadows of the EnlightenmentDa EverandCollective Wisdom in the West: Beyond the shadows of the EnlightenmentNessuna valutazione finora
- Psychological Science in A Postmodern ContextDocumento21 paginePsychological Science in A Postmodern ContextVerónica UrzúaNessuna valutazione finora
- Orientation and Judgment in HermeneuticsDa EverandOrientation and Judgment in HermeneuticsValutazione: 4 su 5 stelle4/5 (1)
- Ahmad Irfan 2024 Sacralising Critique TeDocumento2 pagineAhmad Irfan 2024 Sacralising Critique Tecesar baldiNessuna valutazione finora
- Postmodernism and The Conduct of Inquiry in Social WorkDocumento18 paginePostmodernism and The Conduct of Inquiry in Social WorkKarina Paloma Guerra PintoNessuna valutazione finora
- Philosophical Objections To The Knowability of TruthDocumento8 paginePhilosophical Objections To The Knowability of TruthRasheed ArshadNessuna valutazione finora
- Nordicom ReviewDocumento9 pagineNordicom ReviewIvánJuárezNessuna valutazione finora
- Foucault & Turn To Narrative TherapyDocumento19 pagineFoucault & Turn To Narrative TherapyJuan AntonioNessuna valutazione finora
- 1 Postmodern Poststructural Therapy OverviewDocumento19 pagine1 Postmodern Poststructural Therapy OverviewEllia WatersNessuna valutazione finora
- Collaborative Therapy Relationships and Conversations That Make A DifferenceDocumento25 pagineCollaborative Therapy Relationships and Conversations That Make A Differenceisiplaya2013Nessuna valutazione finora
- Inherent Self, Invented Self, Empty Self: Constructivism, Buddhism, and PsychotherapyDocumento22 pagineInherent Self, Invented Self, Empty Self: Constructivism, Buddhism, and PsychotherapyNarcisNessuna valutazione finora
- Epstein, E. The Narrative Turn Postmodern Theory and Systemic TherapyDocumento10 pagineEpstein, E. The Narrative Turn Postmodern Theory and Systemic TherapyEugene EpsteinNessuna valutazione finora
- Postmodernism, Constructionism and The Idea of Reality:: A Contribution To The 'Ism' DiscussionsDocumento4 paginePostmodernism, Constructionism and The Idea of Reality:: A Contribution To The 'Ism' DiscussionsTasos TravasarosNessuna valutazione finora
- ModernTruthandPostmodernIncredulity IJRMDocumento14 pagineModernTruthandPostmodernIncredulity IJRMDesi NoobsNessuna valutazione finora
- Intersections of Feminist and Transpersonal ThoughtDocumento25 pagineIntersections of Feminist and Transpersonal ThoughtInternational Journal of Transpersonal StudiesNessuna valutazione finora
- A Typology of RitualDocumento16 pagineA Typology of RitualpiekamarekNessuna valutazione finora
- Zeitgeist ThesisDocumento7 pagineZeitgeist ThesisSara Parker100% (2)
- Spivak KDocumento326 pagineSpivak KseNessuna valutazione finora
- Literacy, Critical Article (Longer Version)Documento22 pagineLiteracy, Critical Article (Longer Version)Carlos Renato LopesNessuna valutazione finora
- Accessav13n2 082Documento13 pagineAccessav13n2 082Samreen KhanNessuna valutazione finora
- Des vs. Interpretative PhenoDocumento28 pagineDes vs. Interpretative PhenoMarwin ObmergaNessuna valutazione finora
- From The Hermeneutics of Traditions To The History of Ideas in The Context of OralityDocumento31 pagineFrom The Hermeneutics of Traditions To The History of Ideas in The Context of OralitymarcosclopesNessuna valutazione finora
- GR 1103 EvansDocumento14 pagineGR 1103 EvansJoão Vitor Moreira MaiaNessuna valutazione finora
- Tod and The Caring City - LmsDocumento15 pagineTod and The Caring City - LmslauramenzalNessuna valutazione finora
- On Research Worthy of The Present 2019 PDFDocumento13 pagineOn Research Worthy of The Present 2019 PDFAnonymous slVH85zYNessuna valutazione finora
- Posmodernidade EspiritudalidadeDocumento20 paginePosmodernidade EspiritudalidadeManoel SimaoNessuna valutazione finora
- Jurisprudence II 4.5.2010 AssignmentDocumento2 pagineJurisprudence II 4.5.2010 Assignmentmary4hisgloryNessuna valutazione finora
- The Assault Against Logic by Steve YatesDocumento28 pagineThe Assault Against Logic by Steve YatesDeea MilanNessuna valutazione finora
- Studstill Mystical Pluralist Theory of Mysticism in The Unity of Mystical Traditions PP 1 34Documento42 pagineStudstill Mystical Pluralist Theory of Mysticism in The Unity of Mystical Traditions PP 1 34vstevealexanderNessuna valutazione finora
- Fine, M. (2007) Expanding The Methodological ImaginationDocumento15 pagineFine, M. (2007) Expanding The Methodological ImaginationiamnotsupermanhahahaNessuna valutazione finora
- John Gale - Inscription Into The Community. A Footnote On A Lacanian Approach To The Group Treatment of PsychosisDocumento13 pagineJohn Gale - Inscription Into The Community. A Footnote On A Lacanian Approach To The Group Treatment of PsychosisMarija SimonovicNessuna valutazione finora
- Graffiti Between Détournement and Co-OptationDocumento64 pagineGraffiti Between Détournement and Co-OptationAlexandra Sleepalot100% (1)
- Pentecostalism and Shamanism in Asia and Beyond: An Inter-Disciplinary AnalysisDocumento68 paginePentecostalism and Shamanism in Asia and Beyond: An Inter-Disciplinary AnalysisMax anykeyNessuna valutazione finora
- Method or Madness: Transcendental Phenomenology As Knowledge CreatorDocumento41 pagineMethod or Madness: Transcendental Phenomenology As Knowledge CreatorPsychologyEnergyNessuna valutazione finora
- Stiegler Anthropocene and NeganthropologyDocumento16 pagineStiegler Anthropocene and NeganthropologyPatricia TovarNessuna valutazione finora
- Narrative Approaches To Case StudiesDocumento56 pagineNarrative Approaches To Case Studiesgar2toneNessuna valutazione finora
- Hoffman - An Art of LensesDocumento7 pagineHoffman - An Art of LensesSelma Fidalgo CardosoNessuna valutazione finora
- Art Terapie AdhdDocumento11 pagineArt Terapie AdhdsimNessuna valutazione finora
- Structuralism, Post-Structuralism and Post-ModernismDocumento6 pagineStructuralism, Post-Structuralism and Post-ModernismPaloma RoblesNessuna valutazione finora
- Qualitative and Quantitative Dichotomy in ResearchDocumento4 pagineQualitative and Quantitative Dichotomy in ResearchRay John DulapNessuna valutazione finora
- Theology in A Postmodern Culture - Ten Challenges - G. J. Rossouw 1993Documento14 pagineTheology in A Postmodern Culture - Ten Challenges - G. J. Rossouw 1993Feng WeiNessuna valutazione finora
- Collaborative Inquiry Chapter 22 Gehart Tarragona Bava PDFDocumento12 pagineCollaborative Inquiry Chapter 22 Gehart Tarragona Bava PDFnicolas mossoNessuna valutazione finora
- Communicative VirtuosityDocumento27 pagineCommunicative VirtuosityAndrea LinardiNessuna valutazione finora
- Action Morality and Cultural TranslationDocumento29 pagineAction Morality and Cultural TranslationJai SinghNessuna valutazione finora
- Constructing Realities: An Art of Lenses: 44 Summer ST., North Amherst MA 01059Documento8 pagineConstructing Realities: An Art of Lenses: 44 Summer ST., North Amherst MA 01059Betzi RuizNessuna valutazione finora
- FulltextDocumento16 pagineFulltextAnderson BerbesiNessuna valutazione finora
- Complexity in EEDocumento14 pagineComplexity in EELuis Mario MendeléyevNessuna valutazione finora
- Rhodes Narratives 2017Documento9 pagineRhodes Narratives 2017Naxo SepulvedaNessuna valutazione finora
- Rhetorics of Physical TherapyDocumento10 pagineRhetorics of Physical TherapyMiks BrasliņšNessuna valutazione finora
- Standpoint Theory, Situated Knowledge and The Situated ImaginationDocumento19 pagineStandpoint Theory, Situated Knowledge and The Situated ImaginationLorpaNessuna valutazione finora
- MorawskiDocumento10 pagineMorawskiecdafNessuna valutazione finora
- From Kant To Popper: Reason and Critical Rationalism in Organization StudiesDocumento19 pagineFrom Kant To Popper: Reason and Critical Rationalism in Organization StudiesJheanne KimNessuna valutazione finora
- Epistemology Thesis TopicsDocumento5 pagineEpistemology Thesis TopicsAcademicPaperWritersUK100% (2)
- Crash Modernism Meets Postmodernism in CounselingDocumento8 pagineCrash Modernism Meets Postmodernism in CounselingJangHendiNessuna valutazione finora
- Saray Khumalo Goes Big To Mark World Literacy DayDocumento2 pagineSaray Khumalo Goes Big To Mark World Literacy DayLCNessuna valutazione finora
- Tourism Fund Brochure (New Generation)Documento4 pagineTourism Fund Brochure (New Generation)LCNessuna valutazione finora
- Global Citizen - Africa Fellowship Programme Media ReleaseDocumento2 pagineGlobal Citizen - Africa Fellowship Programme Media ReleaseLCNessuna valutazione finora
- White Star Steps in To Keep The Beat Alive!Documento2 pagineWhite Star Steps in To Keep The Beat Alive!LCNessuna valutazione finora
- Empowerment Brochure (New Generation)Documento4 pagineEmpowerment Brochure (New Generation)LCNessuna valutazione finora
- Lockdown Restrictions Eased, But TV Is Still KingDocumento2 pagineLockdown Restrictions Eased, But TV Is Still KingLCNessuna valutazione finora
- Faces of Business Partners: Business ExpansionsDocumento1 paginaFaces of Business Partners: Business ExpansionsLCNessuna valutazione finora
- Faces of Business Partners: Start-UpsDocumento1 paginaFaces of Business Partners: Start-UpsLCNessuna valutazione finora
- Bridget Masinga: ProfileDocumento2 pagineBridget Masinga: ProfileLCNessuna valutazione finora
- Saray Khumalo: Listicle (Women and Purpose)Documento2 pagineSaray Khumalo: Listicle (Women and Purpose)LCNessuna valutazione finora
- Vuyo's Funerals: Social Media Post (Funeral Rituals)Documento2 pagineVuyo's Funerals: Social Media Post (Funeral Rituals)LCNessuna valutazione finora
- Vuyo's Funerals - Media Release (GBV)Documento2 pagineVuyo's Funerals - Media Release (GBV)LCNessuna valutazione finora
- Brand SA - Africa Day Media ReleaseDocumento3 pagineBrand SA - Africa Day Media ReleaseLCNessuna valutazione finora
- SA Book Fair - Media Release (Programme Highlights) (Literary Media) V5 180705 (Final)Documento4 pagineSA Book Fair - Media Release (Programme Highlights) (Literary Media) V5 180705 (Final)LCNessuna valutazione finora
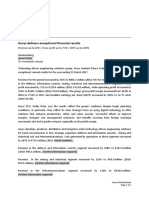
- Ansys - IR 2016 Defence and Information SectorDocumento3 pagineAnsys - IR 2016 Defence and Information SectorLCNessuna valutazione finora
- Ansys - Media Release (Cybersecurity)Documento2 pagineAnsys - Media Release (Cybersecurity)LCNessuna valutazione finora
- Genesis Analytics - FS Mailer (Commodities)Documento1 paginaGenesis Analytics - FS Mailer (Commodities)LCNessuna valutazione finora
- White Star - SABiggestBreakfast Media ReleaseDocumento2 pagineWhite Star - SABiggestBreakfast Media ReleaseLCNessuna valutazione finora
- Global Citizen - Africa Fellowship Programme Media ReleaseDocumento2 pagineGlobal Citizen - Africa Fellowship Programme Media ReleaseLCNessuna valutazione finora
- Ansys - IR 2016 Telecoms Sector OverviewDocumento2 pagineAnsys - IR 2016 Telecoms Sector OverviewLCNessuna valutazione finora
- CareersSA Graduate ProfilesDocumento9 pagineCareersSA Graduate ProfilesLCNessuna valutazione finora
- The Paper StoryDocumento5 pagineThe Paper StoryLCNessuna valutazione finora
- Vhukoni Incentive Programme Web Site Copy: Welcome To Vhukoni! (Home Page)Documento6 pagineVhukoni Incentive Programme Web Site Copy: Welcome To Vhukoni! (Home Page)LCNessuna valutazione finora
- Ansys - Shareholder and Analyst NewsletterDocumento2 pagineAnsys - Shareholder and Analyst NewsletterLCNessuna valutazione finora
- MPA - DTI EditorialDocumento3 pagineMPA - DTI EditorialLCNessuna valutazione finora
- SASRIA - Executive SpeechDocumento2 pagineSASRIA - Executive SpeechLCNessuna valutazione finora
- Ansys - Empowerdex Q&ADocumento3 pagineAnsys - Empowerdex Q&ALCNessuna valutazione finora
- Ansys - Media Release (Annual Results Y2017)Documento2 pagineAnsys - Media Release (Annual Results Y2017)LCNessuna valutazione finora
- Global Citizen - Siya Kolisi AnnouncementDocumento7 pagineGlobal Citizen - Siya Kolisi AnnouncementLCNessuna valutazione finora
- Etion - Corporate Profile (JSE Magazine)Documento1 paginaEtion - Corporate Profile (JSE Magazine)LCNessuna valutazione finora
- CAS Supervisor FormDocumento4 pagineCAS Supervisor FormAskiya ThaparNessuna valutazione finora
- Assessment in SchoolsDocumento169 pagineAssessment in SchoolsCletus Batton100% (1)
- Mini Mental State - A Practical Method For Grading The Cognitive State of Patients For The ClinicianDocumento10 pagineMini Mental State - A Practical Method For Grading The Cognitive State of Patients For The ClinicianIvana FasanoNessuna valutazione finora
- TOS 3rdqtr FABM2Documento5 pagineTOS 3rdqtr FABM2Rossano DavidNessuna valutazione finora
- DiassDocumento34 pagineDiassSOUTH PAWNessuna valutazione finora
- Ethics Quizzes - CHPT 4Documento9 pagineEthics Quizzes - CHPT 4Branden Monfreda50% (6)
- An Insiders Guide To Sub-Modalities - Richard BandlerDocumento127 pagineAn Insiders Guide To Sub-Modalities - Richard Bandlerjacobpalmer100% (15)
- Befikadu Taye PDFDocumento91 pagineBefikadu Taye PDFAll Rights ReservedNessuna valutazione finora
- Tip 5Documento3 pagineTip 5api-454303170Nessuna valutazione finora
- Thesis 12Documento15 pagineThesis 12Aurea Ladera-Pasion67% (3)
- Behavior Rating Inventory of Executive Function RDocumento7 pagineBehavior Rating Inventory of Executive Function RTZU chi LiuNessuna valutazione finora
- MANIADocumento1 paginaMANIALillabinNessuna valutazione finora
- Emotional ManipulatorsDocumento12 pagineEmotional ManipulatorsKarina Yesenia Salinas100% (2)
- Adult Learner InterviewDocumento5 pagineAdult Learner Interviewapi-279420767Nessuna valutazione finora
- Instructions:: Module 2-Learning Activity 1 (M 2-LA1) August 16, 2021Documento2 pagineInstructions:: Module 2-Learning Activity 1 (M 2-LA1) August 16, 2021BARBO, KIMBERLY T.Nessuna valutazione finora
- OCD - Key Facts"Documento3 pagineOCD - Key Facts"Santosh ParabNessuna valutazione finora
- Allama Iqbal Open University (Department of Business Administration)Documento6 pagineAllama Iqbal Open University (Department of Business Administration)Khawaja SabirNessuna valutazione finora
- Individual Activity 3: NSTP 1 - Self Awareness & Values DevelopmentDocumento2 pagineIndividual Activity 3: NSTP 1 - Self Awareness & Values DevelopmentMaylyn TubieronNessuna valutazione finora
- SleepDocumento28 pagineSleepshehina mNessuna valutazione finora
- 1 PBDocumento12 pagine1 PBPinj BlueNessuna valutazione finora
- FossilizationDocumento4 pagineFossilizationKrySt TeyNessuna valutazione finora
- Review On Institutional CorrectionsDocumento15 pagineReview On Institutional Correctionscriminologyalliance83% (6)
- Theoriess - Mr. BajetDocumento61 pagineTheoriess - Mr. BajetMaria Cristina DelmoNessuna valutazione finora
- Procrastination, Perfectionism, and Other Work-Related Mental ProblemsDocumento12 pagineProcrastination, Perfectionism, and Other Work-Related Mental ProblemsFrancisco MartinezNessuna valutazione finora
- Presentation - 0Documento12 paginePresentation - 0Mvrx XventhNessuna valutazione finora
- Performance Management & Appraisals Project ReportDocumento19 paginePerformance Management & Appraisals Project Reportkamdica100% (6)
- Self EvaluationDocumento2 pagineSelf Evaluationapi-359782139Nessuna valutazione finora
- Summary EYl 10Documento3 pagineSummary EYl 10Afifah Hisyam BachmidNessuna valutazione finora
- PRACTICALDocumento14 paginePRACTICALaltherjameseleazarNessuna valutazione finora
- Organisational ChartDocumento2 pagineOrganisational Chartapi-366102737Nessuna valutazione finora
- The Age of Magical Overthinking: Notes on Modern IrrationalityDa EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityValutazione: 4 su 5 stelle4/5 (28)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDa EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionValutazione: 4 su 5 stelle4/5 (404)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDa EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsValutazione: 5 su 5 stelle5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDa EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNessuna valutazione finora
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDa EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedValutazione: 5 su 5 stelle5/5 (81)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDa EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDValutazione: 5 su 5 stelle5/5 (2)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDa EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityValutazione: 4 su 5 stelle4/5 (3)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDa EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDa EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeValutazione: 2 su 5 stelle2/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDa EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsValutazione: 3.5 su 5 stelle3.5/5 (3)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Da EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Nessuna valutazione finora
- The Marshmallow Test: Mastering Self-ControlDa EverandThe Marshmallow Test: Mastering Self-ControlValutazione: 4.5 su 5 stelle4.5/5 (58)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDa EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsValutazione: 4.5 su 5 stelle4.5/5 (170)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningDa EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningValutazione: 4 su 5 stelle4/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDa EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisValutazione: 3.5 su 5 stelle3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDa EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisValutazione: 4 su 5 stelle4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Da EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Valutazione: 4.5 su 5 stelle4.5/5 (110)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Da EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Valutazione: 5 su 5 stelle5/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDa EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessValutazione: 4.5 su 5 stelle4.5/5 (328)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingDa EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingValutazione: 4 su 5 stelle4/5 (1138)
- The Molecule of More: How a Single Chemical in Your Brain Drives Love, Sex, and Creativity--and Will Determine the Fate of the Human RaceDa EverandThe Molecule of More: How a Single Chemical in Your Brain Drives Love, Sex, and Creativity--and Will Determine the Fate of the Human RaceValutazione: 4.5 su 5 stelle4.5/5 (517)
- Summary: Hidden Potential: The Science of Achieving Greater Things By Adam Grant: Key Takeaways, Summary and AnalysisDa EverandSummary: Hidden Potential: The Science of Achieving Greater Things By Adam Grant: Key Takeaways, Summary and AnalysisValutazione: 4.5 su 5 stelle4.5/5 (15)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDa EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryValutazione: 4 su 5 stelle4/5 (44)
- Troubled: A Memoir of Foster Care, Family, and Social ClassDa EverandTroubled: A Memoir of Foster Care, Family, and Social ClassValutazione: 4.5 su 5 stelle4.5/5 (27)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDa EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeValutazione: 4.5 su 5 stelle4.5/5 (253)
- The Secret of the Golden Flower: A Chinese Book Of LifeDa EverandThe Secret of the Golden Flower: A Chinese Book Of LifeValutazione: 5 su 5 stelle5/5 (4)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedDa EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedValutazione: 4 su 5 stelle4/5 (61)