Potrebbero piacerti anche
- Opioid Chapter 2Documento7 pagineOpioid Chapter 2Likoh TimothyNessuna valutazione finora
- Upregulation of Opioid ReceptorsDocumento26 pagineUpregulation of Opioid ReceptorsbrightfutureNessuna valutazione finora
- Treatment of Psychological DisordersDocumento34 pagineTreatment of Psychological DisordersAndreia AlmeidaNessuna valutazione finora
- What Are The Differences Between Psychodynamic Therapy and CBTDocumento5 pagineWhat Are The Differences Between Psychodynamic Therapy and CBTjdc04027Nessuna valutazione finora
- The Multiple Meanings of ADHD Between de PDFDocumento20 pagineThe Multiple Meanings of ADHD Between de PDFRodrigo Guerra ArrauNessuna valutazione finora
- BullyingDocumento9 pagineBullyingGreer LevendalNessuna valutazione finora
- Cognitive DissonanceDocumento15 pagineCognitive DissonancecatalinbryllaNessuna valutazione finora
- Drug Control Master PlanDocumento66 pagineDrug Control Master PlannadeemNessuna valutazione finora
- Is Earlier Sex Education HarmfulDocumento10 pagineIs Earlier Sex Education Harmfulmac202123Nessuna valutazione finora
- The Relationship Between Emotional Intelligence and HappinessDocumento8 pagineThe Relationship Between Emotional Intelligence and HappinessLoredana BarbuNessuna valutazione finora
- Drug AddictionDocumento4 pagineDrug AddictionJessa Danica Costillas ItchonNessuna valutazione finora
- What Is SchizophreniaDocumento19 pagineWhat Is SchizophreniaSheena Arnoco ToraynoNessuna valutazione finora
- NeuronDocumento4 pagineNeuroniris danielle barolaNessuna valutazione finora
- Behavioral Family TherapyDocumento6 pagineBehavioral Family Therapyiulia9gavrisNessuna valutazione finora
- Drugs of Abuse AERDocumento53 pagineDrugs of Abuse AERKayla FrancisNessuna valutazione finora
- Psychosis PDFDocumento34 paginePsychosis PDFGrace LNessuna valutazione finora
- Paradigm Shift FinalDocumento10 pagineParadigm Shift Finalapi-549321056Nessuna valutazione finora
- Substance Abuse Effects On Brain and TreatmentDocumento75 pagineSubstance Abuse Effects On Brain and Treatmentjusq marimarNessuna valutazione finora
- Treatment of Psychological DisordersDocumento32 pagineTreatment of Psychological Disordersfemfen1225100% (2)
- Cognitive Functioning in Adolescents With SelfReported ADHD and Depression Results From A Population-Based StudyDocumento14 pagineCognitive Functioning in Adolescents With SelfReported ADHD and Depression Results From A Population-Based StudyJesúsCoyacNessuna valutazione finora
- Personality Disorders in AsiansDocumento3 paginePersonality Disorders in AsiansIvee van GoghsiaNessuna valutazione finora
- Drug AbuseDocumento15 pagineDrug AbuseGlenn BanlaygasNessuna valutazione finora
- Understanding Substance Abuse in AdolescentsDocumento24 pagineUnderstanding Substance Abuse in AdolescentsJacqueline MansillaNessuna valutazione finora
- Schizophrenia Spectrum and Other Psychotic DisordersDocumento49 pagineSchizophrenia Spectrum and Other Psychotic DisordersNoelle Grace Ulep BaromanNessuna valutazione finora
- Taylor Sowell Drug Report 2017Documento9 pagineTaylor Sowell Drug Report 2017api-457709071Nessuna valutazione finora
- Term Paper On SchizophreniaDocumento25 pagineTerm Paper On SchizophreniaBetlee Ian Barraquias50% (2)
- Schizoaffective DisorderDocumento9 pagineSchizoaffective DisorderIka KawaiiNessuna valutazione finora
- Long Term Pharmacotherapy For Alcohol Dependence: Centre of Addiction Medicine NIMHANS, BangaloreDocumento55 pagineLong Term Pharmacotherapy For Alcohol Dependence: Centre of Addiction Medicine NIMHANS, BangaloreGirish NagarNessuna valutazione finora
- Theories of Personality and Personality Disorders - Heim - Textbook of Pers Disorders 2005Documento41 pagineTheories of Personality and Personality Disorders - Heim - Textbook of Pers Disorders 2005Amira Abdul Wahid100% (1)
- Case Studies Diagnostic LabDocumento3 pagineCase Studies Diagnostic LabAngad AnandNessuna valutazione finora
- ABPSYDocumento15 pagineABPSYBi TchNessuna valutazione finora
- Eradicating Ignorance: J. Rupke ENGL 151-023 M. Walker Dec 04, 2012Documento9 pagineEradicating Ignorance: J. Rupke ENGL 151-023 M. Walker Dec 04, 2012jasonrupkeNessuna valutazione finora
- Working Group On Psychotropic MedicationDocumento246 pagineWorking Group On Psychotropic MedicationAna LópezNessuna valutazione finora
- Fitzgerald - Child Psychoanalytic PsychotherapyDocumento8 pagineFitzgerald - Child Psychoanalytic PsychotherapyJulián Alberto Muñoz FigueroaNessuna valutazione finora
- Dementia A Neurodegenerative DisorderDocumento16 pagineDementia A Neurodegenerative DisorderRishabh SinghNessuna valutazione finora
- Aspergers Syndrome Diagnosis and TreatmentDocumento7 pagineAspergers Syndrome Diagnosis and TreatmentTilahun MogesNessuna valutazione finora
- Internet-Based Family Therapy From The Perspective of The Therapist A Qualitative InquiryDocumento219 pagineInternet-Based Family Therapy From The Perspective of The Therapist A Qualitative InquiryDavid Otálvaro Z.Nessuna valutazione finora
- Psychiatric Disorders Associated With EpilepsyDocumento18 paginePsychiatric Disorders Associated With EpilepsyAllan DiasNessuna valutazione finora
- Aggression and AbnormalDocumento9 pagineAggression and AbnormalAbby Orioque IINessuna valutazione finora
- Ap 7Documento3 pagineAp 7Andrea LuraNessuna valutazione finora
- Janet Am J PsychiatDocumento13 pagineJanet Am J PsychiatMaria CarolinaNessuna valutazione finora
- The Role of Diet in Multiple Sclerosis - A ReviewDocumento16 pagineThe Role of Diet in Multiple Sclerosis - A ReviewHabib G. Moutran BarrosoNessuna valutazione finora
- Brain BattalionDocumento27 pagineBrain BattalionJosip JelićNessuna valutazione finora
- Aging and The Brain - The Proceedings of The Fifth Annual Symposium Held ADocumento225 pagineAging and The Brain - The Proceedings of The Fifth Annual Symposium Held AjoaomartinelliNessuna valutazione finora
- Puberty Suppression Medicine or MalpracticeDocumento35 paginePuberty Suppression Medicine or Malpracticebashomatsuo50% (2)
- Alexithymia Body IlusionsDocumento8 pagineAlexithymia Body IlusionsAlex RichieNessuna valutazione finora
- Classical Psychedelics For The Treatment of Depression and AnxietyDocumento14 pagineClassical Psychedelics For The Treatment of Depression and AnxietyAnonymous FjTisojNessuna valutazione finora
- Module 4: Mood Disorders: Disorders and Individuals With Bipolar Disorders. The Key Difference BetweenDocumento7 pagineModule 4: Mood Disorders: Disorders and Individuals With Bipolar Disorders. The Key Difference BetweenLiz Evermore0% (1)
- AbPsych Reviewer 1 PDFDocumento8 pagineAbPsych Reviewer 1 PDFSyndell PalleNessuna valutazione finora
- Changed Processing of Visual Sexual Stimuli Under GnRH-therapy - A Single Case Study in Pedophilia Using Eye Tracking and fMRIDocumento13 pagineChanged Processing of Visual Sexual Stimuli Under GnRH-therapy - A Single Case Study in Pedophilia Using Eye Tracking and fMRIEmy Noviana SandyNessuna valutazione finora
- Adhd PDFDocumento13 pagineAdhd PDFreds_sparksNessuna valutazione finora
- 7.pluralism in Psychiatry PDFDocumento7 pagine7.pluralism in Psychiatry PDFRania ChioureaNessuna valutazione finora
- Drug Law Reform DebateDocumento65 pagineDrug Law Reform DebateLong NgoNessuna valutazione finora
- Artificial Psychology: The Psychology of AIDocumento6 pagineArtificial Psychology: The Psychology of AIAvril19Nessuna valutazione finora
- APA DSM 5 ContentsDocumento9 pagineAPA DSM 5 ContentsRahmi Annisa MaharaniNessuna valutazione finora
- AbpsyDocumento18 pagineAbpsyirish xNessuna valutazione finora
- (2008) Abuse and Dependence Liability of Benzodiazepine-Type DrugsDocumento28 pagine(2008) Abuse and Dependence Liability of Benzodiazepine-Type Drugssharp8787Nessuna valutazione finora
- A Critique of The Dopamine Hypothesis of Schizophrenia and PsychosisDocumento12 pagineA Critique of The Dopamine Hypothesis of Schizophrenia and PsychosisXaviNessuna valutazione finora
- McCutcheon Et Al-2020-World PsychiatryDocumento19 pagineMcCutcheon Et Al-2020-World PsychiatryRob McCutcheonNessuna valutazione finora
- Kapur (2003) Psychosis As A State of Aberrant SalienceDocumento11 pagineKapur (2003) Psychosis As A State of Aberrant SalienceOscar Alejandro Cardenas QuinteroNessuna valutazione finora
- Types of DelusionsDocumento9 pagineTypes of DelusionsGlenn Sampayan100% (1)
- Psychology: (8th Edition, in Modules) David MyersDocumento27 paginePsychology: (8th Edition, in Modules) David Myersmrchubs100% (2)
- Emotional Release Deepak ChopraDocumento4 pagineEmotional Release Deepak ChopraXa SancleNessuna valutazione finora
- Review of Related LiteratureDocumento6 pagineReview of Related LiteratureAlfred Jayson RuizNessuna valutazione finora
- Objective TestsDocumento4 pagineObjective TestsBabita DhruwNessuna valutazione finora
- Selectividad Inglés "Animal Emotions"Documento2 pagineSelectividad Inglés "Animal Emotions"ElisaZhangNessuna valutazione finora
- DSM5 Clasification Diagnostic Criteria Changes PDFDocumento7 pagineDSM5 Clasification Diagnostic Criteria Changes PDFlilomersNessuna valutazione finora
- Huperzia Serrata..........Documento60 pagineHuperzia Serrata..........BíchNguyễnNessuna valutazione finora
- Chapter IiDocumento2 pagineChapter IiRizka HartatiNessuna valutazione finora
- Using Rewards and Sanctions in The Classroom: Pupils' Perceptions of Their Own Responses To Current Behaviour Management StrategiesDocumento4 pagineUsing Rewards and Sanctions in The Classroom: Pupils' Perceptions of Their Own Responses To Current Behaviour Management StrategiesmarlazmarNessuna valutazione finora
- Assignment 3 - Portfolio - Task ListDocumento2 pagineAssignment 3 - Portfolio - Task ListBaonhiiNessuna valutazione finora
- Emotions and Learning: by Reinhard PekrunDocumento32 pagineEmotions and Learning: by Reinhard PekrunTijana VukovićNessuna valutazione finora
- Back Translation MoCA 8.3 Test Versión MexicanaDocumento1 paginaBack Translation MoCA 8.3 Test Versión MexicanaKarolayn MontenegroNessuna valutazione finora
- Sains Humanika: Full PaperDocumento10 pagineSains Humanika: Full PaperShan GovinNessuna valutazione finora
- Basal GangliaDocumento13 pagineBasal GangliaVivek PNessuna valutazione finora
- Pengajuan Judul Skripsi Atas Nama Intan SiregarDocumento54 paginePengajuan Judul Skripsi Atas Nama Intan SiregarIntan SiregarNessuna valutazione finora
- Models of CommunicationDocumento5 pagineModels of CommunicationJoel PagkalinawaNessuna valutazione finora
- Amazing Facts About Our BrainDocumento4 pagineAmazing Facts About Our BrainUmarul FarooqueNessuna valutazione finora
- (Neil Strauss) Emergency This Book Will Save Your (B-Ok - Xyz)Documento9 pagine(Neil Strauss) Emergency This Book Will Save Your (B-Ok - Xyz)Jin VuNessuna valutazione finora
- Erik DigestDocumento4 pagineErik DigestNoemilyn AngelesNessuna valutazione finora
- Teachers Personality and AdjustmentDocumento16 pagineTeachers Personality and AdjustmentsainudheenNessuna valutazione finora
- MCQs NeuroDocumento2 pagineMCQs NeuroBagadi Suneel100% (2)
- Philosophy of SelfDocumento35 paginePhilosophy of Selface date100% (1)
- BVMT-R Manual ReferencesDocumento2 pagineBVMT-R Manual ReferencesCesarNessuna valutazione finora
- Paul Ginns Lectures and Reading DetailsDocumento1 paginaPaul Ginns Lectures and Reading DetailsdiandraNessuna valutazione finora
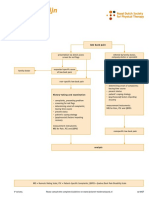
- Dutch LBP Physiotherapy FlowchartDocumento2 pagineDutch LBP Physiotherapy FlowchartyohanNessuna valutazione finora
- Mental Disorders-A MindHeal Homeopathy CaseStudyDocumento2 pagineMental Disorders-A MindHeal Homeopathy CaseStudyDr. Anita SalunkheNessuna valutazione finora
- Motivation & Reward SystemDocumento27 pagineMotivation & Reward SystemLeizel Bajamonde Doblon-ConstantinoNessuna valutazione finora
- PERDEVT BOL 1st QTR SY2020 2021 PDFDocumento12 paginePERDEVT BOL 1st QTR SY2020 2021 PDFRikka EspedillaNessuna valutazione finora
- Vanderbilt ADHD Diagnostic Rating ScaleDocumento2 pagineVanderbilt ADHD Diagnostic Rating ScalevkNessuna valutazione finora