Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Substance Abuse Counseling Complete 5th EditionDocumento379 pagineSubstance Abuse Counseling Complete 5th Editionnintendoagekid86% (59)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- HANDBOOK-McLean-and-Syed-2015-The Oxford Handbook of Identity Development PDFDocumento625 pagineHANDBOOK-McLean-and-Syed-2015-The Oxford Handbook of Identity Development PDFEsp Success Beyond100% (13)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Science ProposalDocumento7 pagineScience ProposalDimple EstelNessuna valutazione finora
- Dr. LakshmayyaDocumento5 pagineDr. LakshmayyanikhilbNessuna valutazione finora
- Hazard Full SlideDocumento31 pagineHazard Full SlideRenKangWongNessuna valutazione finora
- My Good Habits - Welcome Booklet 2 - 1Documento17 pagineMy Good Habits - Welcome Booklet 2 - 1lisa_ernsbergerNessuna valutazione finora
- IPAMS Healthcare and Medical Services Evaluation FormDocumento2 pagineIPAMS Healthcare and Medical Services Evaluation FormManases VelasquezNessuna valutazione finora
- Health Education Plan-DiarrheaDocumento10 pagineHealth Education Plan-DiarrheaMae Dacer50% (2)
- Project Name: Proposed Icomc & BMC Building Complex Phe Design ReportDocumento19 pagineProject Name: Proposed Icomc & BMC Building Complex Phe Design ReportAmit Kumar MishraNessuna valutazione finora
- Crowding Boarding and Patient Through PutDocumento9 pagineCrowding Boarding and Patient Through PutMarwa El SayedNessuna valutazione finora
- Rag WitekDocumento1 paginaRag Witekpkgill15Nessuna valutazione finora
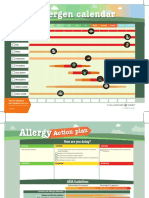
- Allergen Calendar - EnglishDocumento2 pagineAllergen Calendar - Englishpkgill15Nessuna valutazione finora
- Ontario MOHLTC IVIG Request FormDocumento2 pagineOntario MOHLTC IVIG Request Formpkgill15Nessuna valutazione finora
- PFT Req May 11 2016 PDFDocumento1 paginaPFT Req May 11 2016 PDFpkgill15Nessuna valutazione finora
- Mayo Clinic 2009Documento17 pagineMayo Clinic 2009pkgill15Nessuna valutazione finora
- Hemifacial Spasm A NeurosurgicalDocumento8 pagineHemifacial Spasm A NeurosurgicaldnazaryNessuna valutazione finora
- RecormonDocumento36 pagineRecormonShamal FernandoNessuna valutazione finora
- Latest Requirements on Safe Lifting OperationsDocumento22 pagineLatest Requirements on Safe Lifting OperationsThanThanscc100% (1)
- Certification of Psychology Specialists Application Form: Cover PageDocumento3 pagineCertification of Psychology Specialists Application Form: Cover PageJona Mae MetroNessuna valutazione finora
- What Is Drug ReflectionDocumento8 pagineWhat Is Drug ReflectionCeilo TrondilloNessuna valutazione finora
- Written Assignment Unit 7Documento7 pagineWritten Assignment Unit 7Edgar PampulahNessuna valutazione finora
- Mechanical Syllabus PDFDocumento225 pagineMechanical Syllabus PDFshashiNessuna valutazione finora
- Marriage and Later PartDocumento25 pagineMarriage and Later PartDeepak PoudelNessuna valutazione finora
- Health Fair ProposalDocumento2 pagineHealth Fair ProposalElma SintosNessuna valutazione finora
- Roles and Responsibilities of UnderwritingDocumento6 pagineRoles and Responsibilities of UnderwritingShubham DubeyNessuna valutazione finora
- Peripheral Central Giant Cell Granuloma NXPowerLiteDocumento18 paginePeripheral Central Giant Cell Granuloma NXPowerLiteAFREEN SADAF100% (1)
- Hand Injuries & Their ManagementsDocumento78 pagineHand Injuries & Their ManagementsKuruNessuna valutazione finora
- F&F LetterDocumento3 pagineF&F LetterJaskeerat Singh50% (2)
- Pre/Post Test in Mapeh 6 Name: - DateDocumento5 paginePre/Post Test in Mapeh 6 Name: - Datema. rosario yumangNessuna valutazione finora
- Antiparkinsonian Drugs Pathophysiology and TreatmentDocumento5 pagineAntiparkinsonian Drugs Pathophysiology and Treatmentkv 14Nessuna valutazione finora
- BSc Medical Sociology Syllabus DetailsDocumento24 pagineBSc Medical Sociology Syllabus Detailsmchakra72100% (2)
- Hahnemann Advance MethodDocumento2 pagineHahnemann Advance MethodRehan AnisNessuna valutazione finora
- Retyped: CHAP THORNDocumento13 pagineRetyped: CHAP THORNប៉ាក់ ចាន់រ៉ា - Pak ChanraNessuna valutazione finora
- 3.material Science Eng. CDocumento8 pagine3.material Science Eng. CSanjeeb KalitaNessuna valutazione finora
- Research Paper 4Documento26 pagineResearch Paper 4Amit RajputNessuna valutazione finora