Potrebbero piacerti anche
- NCLEX Study MaterialDocumento40 pagineNCLEX Study MaterialChristie GerconNessuna valutazione finora
- Individual Performance Profile PN Nursing Care of Children 2011 Form BDocumento4 pagineIndividual Performance Profile PN Nursing Care of Children 2011 Form BStan Tan67% (3)
- Test Questions From Barbara K. TimbyDocumento5 pagineTest Questions From Barbara K. Timbysuperrhengc0% (1)
- Global Nursing Pediatrics. Nclex - RNDocumento14 pagineGlobal Nursing Pediatrics. Nclex - RNNANANessuna valutazione finora
- LPN DELEGATION and PRIORITIZING AND MOREDocumento38 pagineLPN DELEGATION and PRIORITIZING AND MOREDebra PowellNessuna valutazione finora
- Random NCLEX Tips 101 AileenDocumento9 pagineRandom NCLEX Tips 101 AileenxaileenxNessuna valutazione finora
- Nclex-Pn Chapter 21 BwfinalDocumento12 pagineNclex-Pn Chapter 21 BwfinalatmojdNessuna valutazione finora
- Gastrointestinal: Nclex-Rn ReviewerDocumento34 pagineGastrointestinal: Nclex-Rn ReviewerJohnasse Sebastian NavalNessuna valutazione finora
- Bullets Nclex Terms 50Documento48 pagineBullets Nclex Terms 50ShazaNessuna valutazione finora
- NCLEX-RN Test Plan (Detailed Candiate Version)Documento62 pagineNCLEX-RN Test Plan (Detailed Candiate Version)Filipino Nurses CentralNessuna valutazione finora
- Answers and Rationales For NCLEX Style Review QuestionsDocumento12 pagineAnswers and Rationales For NCLEX Style Review QuestionsJacinth Florido Fedelin50% (2)
- 56: Neurological System: Practice QuestionsDocumento36 pagine56: Neurological System: Practice Questionsjutah2013Nessuna valutazione finora
- Immunity 1Documento6 pagineImmunity 1Tori RolandNessuna valutazione finora
- Vati FundsDocumento2 pagineVati FundsAudrey WatsonNessuna valutazione finora
- NCLEX Study GuideDocumento35 pagineNCLEX Study Guidedchirinos90100% (1)
- Nclex RN Sata CompilationDocumento10 pagineNclex RN Sata CompilationJanna mae PatriarcaNessuna valutazione finora
- 2016module5 PDFDocumento24 pagine2016module5 PDFAicir Tap100% (1)
- Q&A Psychocosocial 1Documento12 pagineQ&A Psychocosocial 1api-3818438Nessuna valutazione finora
- Hurst Review CDC Infection Control ChartDocumento44 pagineHurst Review CDC Infection Control ChartTerry Thun100% (2)
- When Can I Register For The NCLEX-RN Exam?Documento3 pagineWhen Can I Register For The NCLEX-RN Exam?mimNessuna valutazione finora
- NCLEXDocumento3 pagineNCLEXEternity RealNessuna valutazione finora
- NCLEX RNdemo PDFDocumento14 pagineNCLEX RNdemo PDFHarrington KalumbwaNessuna valutazione finora
- NCLEX Study GuideDocumento7 pagineNCLEX Study Guidemmgoodall22100% (3)
- Maternal and Child Nursing Care 3rd Edition London Test BankDocumento11 pagineMaternal and Child Nursing Care 3rd Edition London Test BankSerenaNessuna valutazione finora
- View AnswersDocumento4 pagineView AnswersFaith Levi Alecha AlferezNessuna valutazione finora
- Compiled Nclex Tips and QuestionsDocumento99 pagineCompiled Nclex Tips and QuestionsPaolo Balon100% (2)
- Nclex Question Answers With Rationale - April 2018Documento7 pagineNclex Question Answers With Rationale - April 2018javedNessuna valutazione finora
- Nclex RN Demo 170705092947Documento13 pagineNclex RN Demo 170705092947padma100% (2)
- Nclex ExamDocumento47 pagineNclex Examdamn-regret-1955Nessuna valutazione finora
- NCLEX Helpful HintsDocumento2 pagineNCLEX Helpful HintsJamie Antonini GrantNessuna valutazione finora
- NCLEX Test Taking TipsDocumento3 pagineNCLEX Test Taking TipsjrilleraNessuna valutazione finora
- Content of The NclexDocumento8 pagineContent of The NclexHerkulanus ErwinNessuna valutazione finora
- RNDocumento16 pagineRNrunnermn100% (1)
- Test-Taking Tips For NCLEXDocumento59 pagineTest-Taking Tips For NCLEXJbl2328Nessuna valutazione finora
- Review Program DescriptionDocumento8 pagineReview Program Descriptionnanchie100% (3)
- ATI Comprehensive Predictor: Study Online atDocumento9 pagineATI Comprehensive Predictor: Study Online atVanessaMUellerNessuna valutazione finora
- ReMar Nurse University 2020 (VT) Student WorkbookDocumento50 pagineReMar Nurse University 2020 (VT) Student WorkbookAnderson AlfredNessuna valutazione finora
- Q&A PrioritizationDocumento12 pagineQ&A Prioritizationapi-3818438Nessuna valutazione finora
- Select All That ApplyDocumento10 pagineSelect All That ApplyJohnasse Sebastian NavalNessuna valutazione finora
- Strategy DefinitionsDocumento8 pagineStrategy DefinitionskwameNessuna valutazione finora
- NCLEXDocumento95 pagineNCLEXrikkapupuNessuna valutazione finora
- 52 Nclex ReviewDocumento1 pagina52 Nclex ReviewedobleNessuna valutazione finora
- Exam 3 Review Med SurgDocumento18 pagineExam 3 Review Med SurgCarol ReidNessuna valutazione finora
- NCLEX Study GuideDocumento2 pagineNCLEX Study GuideLogin Nurse100% (1)
- Week 3 Nclex ReviewDocumento71 pagineWeek 3 Nclex Reviewmelissamichellle50% (2)
- NCLEX Review ExamplefinalDocumento52 pagineNCLEX Review Examplefinalisapatrick8126100% (1)
- Check My Twitter Account @nursetopia or IG @nursetopia1 For More Nursing Test Banks, Sample Exam, Reviewers, and NotesDocumento5 pagineCheck My Twitter Account @nursetopia or IG @nursetopia1 For More Nursing Test Banks, Sample Exam, Reviewers, and NotesNurse UtopiaNessuna valutazione finora
- Nclex Question and Rationale Week 4Documento10 pagineNclex Question and Rationale Week 4Winnie Okoth100% (1)
- Chapter 41: The Child With An Infectious Disease Test Bank: Multiple ChoiceDocumento10 pagineChapter 41: The Child With An Infectious Disease Test Bank: Multiple ChoiceNurse UtopiaNessuna valutazione finora
- Nclex 3500Documento4 pagineNclex 3500chitorNessuna valutazione finora
- NCLEX Updates June 2010Documento21 pagineNCLEX Updates June 2010erika_datu100% (1)
- Mark K Lecture #2Documento16 pagineMark K Lecture #2Melissa Sapp100% (2)
- RPN Priority and Delegation TestDocumento5 pagineRPN Priority and Delegation Testfairwoods0% (2)
- Hesi Med Surg-14Documento1 paginaHesi Med Surg-14GeorgeNessuna valutazione finora
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideDa EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNessuna valutazione finora
- PN FUNDAMENTALS: Passbooks Study GuideDa EverandPN FUNDAMENTALS: Passbooks Study GuideNessuna valutazione finora
- NURSING CARE OF ADULTS I: Passbooks Study GuideDa EverandNURSING CARE OF ADULTS I: Passbooks Study GuideNessuna valutazione finora
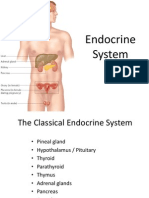
- Endocrine SystemDocumento96 pagineEndocrine SystemSandhya Kakkar100% (3)
- Adrenocortical DisordersDocumento73 pagineAdrenocortical DisordersReunita ConstantiaNessuna valutazione finora
- Adrenal GlandDocumento2 pagineAdrenal GlandAurelia AlexandraNessuna valutazione finora
- All Emqs Saqs Sample QsDocumento12 pagineAll Emqs Saqs Sample QsSanathRaoNessuna valutazione finora
- Hypertension in The Dog and Cat PDFDocumento374 pagineHypertension in The Dog and Cat PDFaLÔ REGINANessuna valutazione finora
- Adrenal Glands 2018 - 2019Documento32 pagineAdrenal Glands 2018 - 2019Bianca BiaNessuna valutazione finora
- Primary AldosteronismDocumento5 paginePrimary AldosteronismIfeanyichukwu OgbonnayaNessuna valutazione finora
- Flash Pulmonary Oedema and Bilateral Renal Artery Stenosis: The Pickering SyndromeDocumento8 pagineFlash Pulmonary Oedema and Bilateral Renal Artery Stenosis: The Pickering SyndromeMahmoud DiaaNessuna valutazione finora
- Lkbsis53 Potassium 30343Documento2 pagineLkbsis53 Potassium 30343nmakrygNessuna valutazione finora
- Disease of Adrenal GlandDocumento47 pagineDisease of Adrenal GlandgibreilNessuna valutazione finora
- Jurnal KesehatanDocumento10 pagineJurnal KesehatanNurul AiniNessuna valutazione finora
- Low Free T4 Normal Free T4 High Free T4Documento3 pagineLow Free T4 Normal Free T4 High Free T4Joseph De JoyaNessuna valutazione finora
- Ch-13 Drugs Used in Heart FailureDocumento49 pagineCh-13 Drugs Used in Heart FailureShabrin SadikhNessuna valutazione finora
- NCM103 12th Endoc IIDocumento9 pagineNCM103 12th Endoc IIKamx MohammedNessuna valutazione finora
- Aldosterone Renin RatioDocumento2 pagineAldosterone Renin RatioPoon CaniceNessuna valutazione finora
- Nursing Care of Adults: Metabolic and Endocrine DisordersDocumento134 pagineNursing Care of Adults: Metabolic and Endocrine DisordersMary Ann Pardilla Alcober100% (4)
- Assignment of Adrenal CortexDocumento12 pagineAssignment of Adrenal CortexWania AliNessuna valutazione finora
- Regulation of ElectrolytesDocumento28 pagineRegulation of ElectrolytesnirilibNessuna valutazione finora
- HemodialysisDocumento58 pagineHemodialysisPamela Joy Seriosa100% (1)
- Anatomy and Physiology PDFDocumento51 pagineAnatomy and Physiology PDFalexenneth canilaNessuna valutazione finora
- Renal Artery StenosisDocumento80 pagineRenal Artery StenosisAnn FloydNessuna valutazione finora
- Fluid and Electrolytes Lecture NotesDocumento85 pagineFluid and Electrolytes Lecture NotesVince Peliño De MesaNessuna valutazione finora
- Rauvolfia Serpentina L. Benth. Ex Kurz.: Phytochemical, Pharmacological andDocumento8 pagineRauvolfia Serpentina L. Benth. Ex Kurz.: Phytochemical, Pharmacological andFarisi RazakNessuna valutazione finora
- Chapter 37 Berne and LevyDocumento4 pagineChapter 37 Berne and LevyJoezelleNessuna valutazione finora
- Renal Tubular AcidosisDocumento6 pagineRenal Tubular AcidosisRichella Khansa Lauditta100% (1)
- The Renin-Angiotensin Aldosterone System: Pathophysiological Role and Pharmacologic InhibitionDocumento12 pagineThe Renin-Angiotensin Aldosterone System: Pathophysiological Role and Pharmacologic Inhibitionfatimah hasibuanNessuna valutazione finora
- What Does High Potassium in Blood Work MeanDocumento2 pagineWhat Does High Potassium in Blood Work MeanMathumathi BalakrishnanNessuna valutazione finora
- Homeostasis and ExcretionDocumento35 pagineHomeostasis and ExcretionronaldwepukhuluNessuna valutazione finora
- Physio 4.7 H2O & Electrolytes Regulation, Micturition Reflex & Urinalysis - JerezDocumento5 paginePhysio 4.7 H2O & Electrolytes Regulation, Micturition Reflex & Urinalysis - Jerezlovelots1234Nessuna valutazione finora
- Glanela Manaloto: Clinical ChemistryDocumento48 pagineGlanela Manaloto: Clinical ChemistryGlanela M. BenjaminNessuna valutazione finora