Potrebbero piacerti anche
- Pharmacological Management of Type 2 Diabetes Mellitus: Rationale For Rational Use of InsulinDocumento9 paginePharmacological Management of Type 2 Diabetes Mellitus: Rationale For Rational Use of InsulinAditya Rachman Van Der ArjunaqueeNessuna valutazione finora
- ADA - UKPD StudyDocumento5 pagineADA - UKPD StudyMagdalena MercyanaNessuna valutazione finora
- Gudoy, Charies Jamille 12-WeierstrassDocumento4 pagineGudoy, Charies Jamille 12-WeierstrasschaNessuna valutazione finora
- Combination Treatment With Insulin and Oral Agents in Type 2 Diabetes MellitusDocumento6 pagineCombination Treatment With Insulin and Oral Agents in Type 2 Diabetes MellitusEstiPramestiningtyasNessuna valutazione finora
- British Journal of Diabetes & Vascular Disease-2006-Pratley-150-6Documento8 pagineBritish Journal of Diabetes & Vascular Disease-2006-Pratley-150-6Nurul FajrinaNessuna valutazione finora
- L Tiple: Përgjigje-Kumar&Clark 'S Clinical MedicineDocumento10 pagineL Tiple: Përgjigje-Kumar&Clark 'S Clinical MedicineNreca TokjonaNessuna valutazione finora
- DM Type 2 Practice EssentialsDocumento31 pagineDM Type 2 Practice Essentialskuchaibaru90Nessuna valutazione finora
- Update On Insulin Therapy For Type 2 DiabetesDocumento9 pagineUpdate On Insulin Therapy For Type 2 DiabetesRIKANessuna valutazione finora
- Clinical Review 102 Type 2 Diabetes Mellitus: Update On Diagnosis, Pathophysiology, and TreatmentDocumento7 pagineClinical Review 102 Type 2 Diabetes Mellitus: Update On Diagnosis, Pathophysiology, and TreatmentWyn AgustinNessuna valutazione finora
- Alternative Therapies For DM 2Documento14 pagineAlternative Therapies For DM 2Ferc27Nessuna valutazione finora
- Insulin Therapy For Type 2 Diabetes Mellitus.Documento11 pagineInsulin Therapy For Type 2 Diabetes Mellitus.Clarissa CozziNessuna valutazione finora
- Hypoglycemia in Diabetes: P E. C, S N. D, H SDocumento11 pagineHypoglycemia in Diabetes: P E. C, S N. D, H SFabio FabbriNessuna valutazione finora
- Type 2 Diabetes MellitusDocumento24 pagineType 2 Diabetes Mellitusdr. M.F. Romdhoni100% (1)
- Canadian: Hypoglycemia: Understanding The EnemyDocumento8 pagineCanadian: Hypoglycemia: Understanding The EnemyndistantiNessuna valutazione finora
- DeFronzo PDFDocumento23 pagineDeFronzo PDFMara HmNessuna valutazione finora
- Screening: DM Tipe 1 Practice EssentialsDocumento20 pagineScreening: DM Tipe 1 Practice Essentialskuchaibaru90Nessuna valutazione finora
- Pathology of Type 2 DiabetesDocumento4 paginePathology of Type 2 DiabetesJenny SembranoNessuna valutazione finora
- Pathogenesis of Type 2 Diabetes Mellitus - UpToDateDocumento26 paginePathogenesis of Type 2 Diabetes Mellitus - UpToDateMelina AranaNessuna valutazione finora
- Kalra 2011Documento7 pagineKalra 2011jinsung parkNessuna valutazione finora
- PMC4020327-jdi 12214Documento11 paginePMC4020327-jdi 12214anca irinaNessuna valutazione finora
- Polypharmacy in The Aging Patient A Review of Glycemic Control in Older Adults With Type 2 DiabetesDocumento12 paginePolypharmacy in The Aging Patient A Review of Glycemic Control in Older Adults With Type 2 Diabetesapi-311409998Nessuna valutazione finora
- Diabetologia: UK Prospective Diabetes Study (UKPDS)Documento14 pagineDiabetologia: UK Prospective Diabetes Study (UKPDS)GuadalupeNessuna valutazione finora
- New Combination Treatments in The Management of Diabetes: Focus On Sitagliptin - MetforminDocumento10 pagineNew Combination Treatments in The Management of Diabetes: Focus On Sitagliptin - MetforminGd PadmawijayaNessuna valutazione finora
- Saxagliptin and Metformin in Fixed Combination For The Treatment of Type 2 Diabetes in AdultsDocumento11 pagineSaxagliptin and Metformin in Fixed Combination For The Treatment of Type 2 Diabetes in AdultsLaura MelatiNessuna valutazione finora
- Initial Management of Blood Glucose in Adults With Type 2 Diabetes Mellitus - UpToDateDocumento24 pagineInitial Management of Blood Glucose in Adults With Type 2 Diabetes Mellitus - UpToDateJessica ArciniegasNessuna valutazione finora
- Ajhp 140168Documento12 pagineAjhp 140168cherrygems99Nessuna valutazione finora
- Intensification of Insulin Therapy in Patients With Type 2 Diabetes Mellitus An Algorithm For Basal Bolus TherapyDocumento12 pagineIntensification of Insulin Therapy in Patients With Type 2 Diabetes Mellitus An Algorithm For Basal Bolus TherapyYudi Fadilah100% (1)
- Dr. Hikmat - Inisiasi Insulin CirebonDocumento44 pagineDr. Hikmat - Inisiasi Insulin CirebonLukman SugiartoNessuna valutazione finora
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesDa EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesValutazione: 4 su 5 stelle4/5 (2)
- Dissertation Diabetes Mellitus Type 2Documento5 pagineDissertation Diabetes Mellitus Type 2Syracuse100% (1)
- Diabetes Mellitus - Type 2 DiabetesDocumento11 pagineDiabetes Mellitus - Type 2 DiabetesHafiz IbrahimNessuna valutazione finora
- Review Inhibition of Dipeptidyl Peptidase-4 With Vildagliptin A Potential New Treatment For Type 2 DiabetesDocumento8 pagineReview Inhibition of Dipeptidyl Peptidase-4 With Vildagliptin A Potential New Treatment For Type 2 DiabetesAndhi FahrurrojiNessuna valutazione finora
- Prediction of Type 2 Diabetes: A Natural History PerspectiveDocumento9 paginePrediction of Type 2 Diabetes: A Natural History Perspectiveandree_zz4890Nessuna valutazione finora
- Diabetes and Cardiovascular Disease: Story of DiscoveryDocumento5 pagineDiabetes and Cardiovascular Disease: Story of DiscoveryMahesh DmNessuna valutazione finora
- Pathogenesis of Type 2 Diabetes Mellitus - UpToDateDocumento38 paginePathogenesis of Type 2 Diabetes Mellitus - UpToDatealinetibes1Nessuna valutazione finora
- Monogenetic Etiologies of DiabetesDocumento12 pagineMonogenetic Etiologies of DiabetesROBERTO RADILLANessuna valutazione finora
- Lec 1Documento9 pagineLec 1fbbqbcht6yNessuna valutazione finora
- Clinical Management of Diabetes in The Elderly: Practical PointersDocumento4 pagineClinical Management of Diabetes in The Elderly: Practical Pointersannaafia69969Nessuna valutazione finora
- Diabetes Obesity Metabolism - 2012 - Stenl F - Efficacy and Safety of Canagliflozin Monotherapy in Subjects With Type 2Documento11 pagineDiabetes Obesity Metabolism - 2012 - Stenl F - Efficacy and Safety of Canagliflozin Monotherapy in Subjects With Type 2Talaat OmranNessuna valutazione finora
- Practice Essentials: Clinical Findings in Diabetes MellitusDocumento14 paginePractice Essentials: Clinical Findings in Diabetes MellituskhonsasyahidahNessuna valutazione finora
- Initial Management of Blood Glucose in Adults With Type 2 Diabetes MellitusDocumento22 pagineInitial Management of Blood Glucose in Adults With Type 2 Diabetes MellitusSaleh M.Nessuna valutazione finora
- Improvement of Insulin Sensitivity in Patients With Type 2 Diabetes Mellitus After Oral Administration of Alpha-Lipoic AcidDocumento8 pagineImprovement of Insulin Sensitivity in Patients With Type 2 Diabetes Mellitus After Oral Administration of Alpha-Lipoic AcidMaghfirahEkasariLaitjinaraNessuna valutazione finora
- Mehanna 2013Documento20 pagineMehanna 2013iacob ancutaNessuna valutazione finora
- Minimizing Hypoglycemia in DiabetesDocumento17 pagineMinimizing Hypoglycemia in DiabetesNovianDwiRoessantiNessuna valutazione finora
- Safari - 26 Jul. 2019 01:14Documento1 paginaSafari - 26 Jul. 2019 01:14Jonathan ZapataNessuna valutazione finora
- Daibetes Mellitus: Dr. Siddaganga S MDocumento45 pagineDaibetes Mellitus: Dr. Siddaganga S Msiddaganga sigiNessuna valutazione finora
- Insulin Therapy in Type 2 Diabetes MellitusDocumento40 pagineInsulin Therapy in Type 2 Diabetes MellitusEDWIN WIJAYANessuna valutazione finora
- Meds DiabetesDocumento5 pagineMeds DiabetesAnjangsari 'aRie' WijayantiNessuna valutazione finora
- Br. J. Anaesth. 2011 Nicholson 65 73Documento9 pagineBr. J. Anaesth. 2011 Nicholson 65 73Adán 'OlveeraNessuna valutazione finora
- Diabetes Mellitus IIDocumento20 pagineDiabetes Mellitus IIMa R Dy100% (1)
- PP Lancet 1998 Ukpds33Documento17 paginePP Lancet 1998 Ukpds33HelloNessuna valutazione finora
- Relapsing and Remitting Insulin Requiring Diabetes: Type 1 or Type 2?Documento2 pagineRelapsing and Remitting Insulin Requiring Diabetes: Type 1 or Type 2?Linda NoveraNessuna valutazione finora
- Diabetes Care 2015Documento8 pagineDiabetes Care 2015Bego ZubietaNessuna valutazione finora
- Informationfordoctors Revised April14Documento2 pagineInformationfordoctors Revised April14Mesfin DerbewNessuna valutazione finora
- Type 2 DMDocumento15 pagineType 2 DMApi HrhpNessuna valutazione finora
- The Control of The Glucose Triad - ChallengesDocumento26 pagineThe Control of The Glucose Triad - ChallengesIoana ZahaNessuna valutazione finora
- Management of Diabetes Mellitus in Patients With Chronic Kidney DiseaseDocumento9 pagineManagement of Diabetes Mellitus in Patients With Chronic Kidney DiseasezakyNessuna valutazione finora
- Garber 2007Documento6 pagineGarber 2007Diana SamuezaNessuna valutazione finora
- Newer Drugs in The Management of Diabetes MellitusDocumento8 pagineNewer Drugs in The Management of Diabetes MellitusAstri Faluna SheylavontiaNessuna valutazione finora
- ED MA: Peman A An Glkoadaahmandii 2021Documento49 pagineED MA: Peman A An Glkoadaahmandii 202119 123 Mohammad SyauqiNessuna valutazione finora
- Insulin Administration)Documento1 paginaInsulin Administration)DanielleNessuna valutazione finora
- Insulin Initiation GuidanceDocumento4 pagineInsulin Initiation GuidanceRahma WatiNessuna valutazione finora
- Inv. Virtual Conference Ryzodeg-16 JAN 2021 - Final - OKDocumento4 pagineInv. Virtual Conference Ryzodeg-16 JAN 2021 - Final - OKmelyekaNessuna valutazione finora
- Anti DiabeticDocumento34 pagineAnti DiabeticEJ GabaoNessuna valutazione finora
- Algorithm For Blood Glucose Lowering Therapy in Adults With Type 2 Diabetes PDF 2185604173Documento1 paginaAlgorithm For Blood Glucose Lowering Therapy in Adults With Type 2 Diabetes PDF 2185604173AlessioNavarraNessuna valutazione finora
- Basal Bolus InsulinDMT22009Documento92 pagineBasal Bolus InsulinDMT22009scribdNessuna valutazione finora
- Insulin Therapy Guide 2Documento3 pagineInsulin Therapy Guide 2AimanRiddleNessuna valutazione finora
- Price List Produk Optima Non Sigma - Per 1 Januari 2021Documento2 paginePrice List Produk Optima Non Sigma - Per 1 Januari 2021yohanes suryonoNessuna valutazione finora
- Humalog Novolog Apidra: Type of Insulin & Brand Names Onset Peak Duration Role in Blood Sugar Management Rapid-ActingDocumento2 pagineHumalog Novolog Apidra: Type of Insulin & Brand Names Onset Peak Duration Role in Blood Sugar Management Rapid-ActingkatrinasdNessuna valutazione finora
- Kelas A Materi I - Terapi Insulin BPJS 2015 (Dr. Makbul)Documento80 pagineKelas A Materi I - Terapi Insulin BPJS 2015 (Dr. Makbul)dr. arsinaNessuna valutazione finora
- Tableau Antidiabetiques 2018 enDocumento1 paginaTableau Antidiabetiques 2018 enpraefatioNessuna valutazione finora
- Anti Diabetik Oral Dan InsulinDocumento97 pagineAnti Diabetik Oral Dan InsulinunknownNessuna valutazione finora
- Diabetes Management & Insulin InitiationDocumento39 pagineDiabetes Management & Insulin InitiationTaufiqurrochman Nur AminNessuna valutazione finora
- Glytrin Brand Plan 2016-17 FinalDocumento54 pagineGlytrin Brand Plan 2016-17 FinalIndranil PoddarNessuna valutazione finora
- Switching Between InsulinDocumento2 pagineSwitching Between InsulinThoufiNessuna valutazione finora
- Tableau Antidiabetiques Guide Des Produits 2017 enDocumento1 paginaTableau Antidiabetiques Guide Des Produits 2017 enHayna RoseNessuna valutazione finora
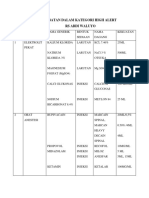
- Obat High AlertDocumento5 pagineObat High AlertChia GracellaNessuna valutazione finora
- Daftar Obat High Alert Dan LasaDocumento1 paginaDaftar Obat High Alert Dan LasaDwinda Juli sandaniNessuna valutazione finora
- Daily Schedule For Type 1 DiabetesDocumento1 paginaDaily Schedule For Type 1 DiabetesMatthew MooreNessuna valutazione finora
- Diabtes MelitusDocumento1 paginaDiabtes Melitusrendi adi saputraNessuna valutazione finora
- Pemberian Insulin KMBDocumento36 paginePemberian Insulin KMBerdhian jatiNessuna valutazione finora
- SESSION 1 Paediatric Insulin Pump Workbook For Children and Young People Living With Type 1 DiabetesDocumento13 pagineSESSION 1 Paediatric Insulin Pump Workbook For Children and Young People Living With Type 1 DiabetesNeema MokobiNessuna valutazione finora
- Oha in Diabetes ManagementDocumento11 pagineOha in Diabetes ManagementAdam HartonoNessuna valutazione finora
- Insulin TypesDocumento3 pagineInsulin TypesAbdullah A. ElgazarNessuna valutazione finora
- Insulin Chart PDFDocumento2 pagineInsulin Chart PDFBapi mirabeau kumbuin100% (1)
- Antihyperglycemic Agents Comparison ChartDocumento9 pagineAntihyperglycemic Agents Comparison ChartBonnieNessuna valutazione finora
- Insulin Guidelines 080114Documento40 pagineInsulin Guidelines 080114ursula_ursulaNessuna valutazione finora
- Insulin Pump - Google SearchDocumento1 paginaInsulin Pump - Google SearchMuhammad Irham syahNessuna valutazione finora
- Insulin InfoDocumento4 pagineInsulin Infomonoj5859Nessuna valutazione finora