Potrebbero piacerti anche
- Anusha Article IJIRMFDocumento5 pagineAnusha Article IJIRMFAnusha SampathNessuna valutazione finora
- Sensorimotor Control Deficiency in Recurrent Anterior Shoulder Instability Assessed With A Stabilometric Force PlatformDocumento6 pagineSensorimotor Control Deficiency in Recurrent Anterior Shoulder Instability Assessed With A Stabilometric Force PlatformA ANessuna valutazione finora
- SciDocumento9 pagineSciCathyCarltonNessuna valutazione finora
- Asj 2020 0146Documento6 pagineAsj 2020 0146Mandeep JangraNessuna valutazione finora
- Pain, Trunk Muscle Strength, Spine Mobility and Disability Following Lumbar Disc SurgeryDocumento5 paginePain, Trunk Muscle Strength, Spine Mobility and Disability Following Lumbar Disc Surgerye7choevaNessuna valutazione finora
- Recovery of Over-Ground Walking After Chronic Motor Complete Spinal Cord InjuryDocumento7 pagineRecovery of Over-Ground Walking After Chronic Motor Complete Spinal Cord Injuryrich sitaNessuna valutazione finora
- Filippi G.M.Documento5 pagineFilippi G.M.berardinoNessuna valutazione finora
- Mikesky EffectsofstrengthtrainingDocumento10 pagineMikesky EffectsofstrengthtrainingArtNessuna valutazione finora
- Va Medica: Effects of Myofascial Technique in Patients With Subacute Whiplash Associated Disorders: A Pilot StudyDocumento0 pagineVa Medica: Effects of Myofascial Technique in Patients With Subacute Whiplash Associated Disorders: A Pilot StudyKaren Jeanette Valderrama CortesNessuna valutazione finora
- The Effects of Scapular Stabilization Based Exercise Therapy On PDFDocumento15 pagineThe Effects of Scapular Stabilization Based Exercise Therapy On PDFElisabete SilvaNessuna valutazione finora
- Physiotherapeutic Intervention in A Patient With Spinal Cord Injury (SCI) .Documento7 paginePhysiotherapeutic Intervention in A Patient With Spinal Cord Injury (SCI) .eka aningNessuna valutazione finora
- Aaa - THAMARA - Comparing Hot Pack, Short-Wave Diathermy, Ultrasound, and Tens On Isokinetic Strength, Pain and Functional StatusDocumento9 pagineAaa - THAMARA - Comparing Hot Pack, Short-Wave Diathermy, Ultrasound, and Tens On Isokinetic Strength, Pain and Functional StatusBruno FellipeNessuna valutazione finora
- Stark 2014Documento9 pagineStark 2014Niken AquariusNessuna valutazione finora
- Glut MedMaxDocumento12 pagineGlut MedMaxColm CoakleyNessuna valutazione finora
- 79b6 PDFDocumento5 pagine79b6 PDFcnsatishNessuna valutazione finora
- Ijpr 2019 163Documento5 pagineIjpr 2019 163Praktek Fisioterapi Mitra SempajaNessuna valutazione finora
- Effects of Neural Mobilization On Pain, Straight Leg Raise Test and Disability in Patients With Radicular Low Back PainDocumento4 pagineEffects of Neural Mobilization On Pain, Straight Leg Raise Test and Disability in Patients With Radicular Low Back PainFallahPhysioNessuna valutazione finora
- Mohan Ty 2016Documento22 pagineMohan Ty 2016M MisbahunnurNessuna valutazione finora
- 2020 Lamberti RCT Effectiveness of RBFT Slow Walking On Mobility in Severe Multiple SclerosisDocumento11 pagine2020 Lamberti RCT Effectiveness of RBFT Slow Walking On Mobility in Severe Multiple SclerosisArmin ParavlićNessuna valutazione finora
- ptrs009 03 03 PDFDocumento6 pagineptrs009 03 03 PDFGusti Ayu KrisnayantiNessuna valutazione finora
- 0269215511423557Documento10 pagine0269215511423557Jose Maria DominguezNessuna valutazione finora
- PGRB SynopsisDocumento21 paginePGRB Synopsis2022824838.pasangNessuna valutazione finora
- E Vects of Three Diverent Training Modalities On The Cross Sectional Area of The Lumbar Multifidus Muscle in Patients With Chronic Low Back PainDocumento6 pagineE Vects of Three Diverent Training Modalities On The Cross Sectional Area of The Lumbar Multifidus Muscle in Patients With Chronic Low Back PainGary LeeNessuna valutazione finora
- Spinal Myo After InjuryDocumento12 pagineSpinal Myo After InjuryVincentius Michael WilliantoNessuna valutazione finora
- A Comparative Study On Effectiveness of Open Versus Closed Kinetic Chain Exercises To Improve Gait in Spastic Diplegic Cerebral PalsyDocumento4 pagineA Comparative Study On Effectiveness of Open Versus Closed Kinetic Chain Exercises To Improve Gait in Spastic Diplegic Cerebral PalsyInternational Journal of PhysiotherapyNessuna valutazione finora
- Lex D de Jong, Pieter U Dijkstra, Johan Gerritsen, Alexander CH Geurts and Klaas PostemaDocumento12 pagineLex D de Jong, Pieter U Dijkstra, Johan Gerritsen, Alexander CH Geurts and Klaas PostemaAnggelia jopa sariNessuna valutazione finora
- Combined Arm Stretch Positioning and Neuromuscular Electrical Stimulation in Patients After Stroke A Random TrialDocumento10 pagineCombined Arm Stretch Positioning and Neuromuscular Electrical Stimulation in Patients After Stroke A Random TrialwahyonoNessuna valutazione finora
- Mjiri 28 87 - 2 PDFDocumento15 pagineMjiri 28 87 - 2 PDFDr Ahmed NabilNessuna valutazione finora
- Effects of Trunk Rehabilitation With Kinesio and Placebo TapingDocumento15 pagineEffects of Trunk Rehabilitation With Kinesio and Placebo TapingShania BaraqbahNessuna valutazione finora
- Case Report Rehabilitation Program in A Patient With A Displaced Femoral Neck FractureDocumento26 pagineCase Report Rehabilitation Program in A Patient With A Displaced Femoral Neck FractureNatalia LoredanaNessuna valutazione finora
- 1385 FullDocumento10 pagine1385 FullSetiaty PandiaNessuna valutazione finora
- Pelvic Muscle Rehabilitation A StandardiDocumento8 paginePelvic Muscle Rehabilitation A StandardiwladjaNessuna valutazione finora
- Ij2023 14Documento7 pagineIj2023 14Julenda CintarinovaNessuna valutazione finora
- Task Oriented Improves Strength - Stroke PatientsDocumento7 pagineTask Oriented Improves Strength - Stroke PatientsPedro FonsecaNessuna valutazione finora
- Research Article: Effects of Low-Level Laser Therapy and Eccentric Exercises in The Treatment of Patellar TendinopathyDocumento7 pagineResearch Article: Effects of Low-Level Laser Therapy and Eccentric Exercises in The Treatment of Patellar TendinopathyAlvin JulianNessuna valutazione finora
- (Folia Medica) Rehabilitation of Patients With Hip Joint Arthroplasty (Late Post-Surgery Period Hospital Rehabilitation)Documento5 pagine(Folia Medica) Rehabilitation of Patients With Hip Joint Arthroplasty (Late Post-Surgery Period Hospital Rehabilitation)manuel velasquezNessuna valutazione finora
- Gait Rehabilitation Spastic HemiparesisDocumento7 pagineGait Rehabilitation Spastic HemiparesisMirna Gallardo ValderramaNessuna valutazione finora
- Case Report Rehabilitation Program in A Patient With Intertrochanteric Femoral FractureDocumento26 pagineCase Report Rehabilitation Program in A Patient With Intertrochanteric Femoral FractureNatalia LoredanaNessuna valutazione finora
- Sex-Related Differences and Effects of Short and LDocumento16 pagineSex-Related Differences and Effects of Short and LMaria Clara BrandãoNessuna valutazione finora
- Evaluation of The Lateral Instability of The Ankle by Inversion Simulation Device and Assessment of The Rehabilitation ProgramDocumento13 pagineEvaluation of The Lateral Instability of The Ankle by Inversion Simulation Device and Assessment of The Rehabilitation ProgramZzDel VerdeNessuna valutazione finora
- Effects of Continuous Passive Motion On Reversing The Adapted Spinal Circuit in Humans With Chronic Spinal Cord InjuryDocumento7 pagineEffects of Continuous Passive Motion On Reversing The Adapted Spinal Circuit in Humans With Chronic Spinal Cord InjuryJoy SantosNessuna valutazione finora
- (31 36) V9N5PTDocumento6 pagine(31 36) V9N5PTASD2019Nessuna valutazione finora
- Heavy-Load Eccentric Calf Muscle Training For The Treatment of Chronic Achilles TendinosisDocumento8 pagineHeavy-Load Eccentric Calf Muscle Training For The Treatment of Chronic Achilles TendinosisburgoschileNessuna valutazione finora
- Assessment of The Anterior Talofibular Ligament Thickness 2017 Journal of MeDocumento5 pagineAssessment of The Anterior Talofibular Ligament Thickness 2017 Journal of MeRyana Fitriana IINessuna valutazione finora
- Brain: Altering Spinal Cord Excitability Enables Voluntary Movements After Chronic Complete Paralysis in HumansDocumento16 pagineBrain: Altering Spinal Cord Excitability Enables Voluntary Movements After Chronic Complete Paralysis in HumansSebastián GallegosNessuna valutazione finora
- 1 s2.0 S1607551X09703614 MainDocumento8 pagine1 s2.0 S1607551X09703614 MainAchenk BarcelonistaNessuna valutazione finora
- Characteristics of Myofascial Pain Syndrome of The Infraspinatus MuscleDocumento9 pagineCharacteristics of Myofascial Pain Syndrome of The Infraspinatus Musclearia tristayanthiNessuna valutazione finora
- Clinical Lumbar Instability and Core Stabilization Exercise: A Literature ReviewDocumento16 pagineClinical Lumbar Instability and Core Stabilization Exercise: A Literature ReviewwladjaNessuna valutazione finora
- Acupuntura para La RodillaDocumento9 pagineAcupuntura para La Rodillaoscarin123456789Nessuna valutazione finora
- A Comparative Study Between Joint Mobilization and Conventional Physiotherapy in Knee OsteoarthritisDocumento4 pagineA Comparative Study Between Joint Mobilization and Conventional Physiotherapy in Knee OsteoarthritisInternational Journal of PhysiotherapyNessuna valutazione finora
- Case Report Rehabilitation Program in Patient With Ankle FractureDocumento26 pagineCase Report Rehabilitation Program in Patient With Ankle FractureNatalia LoredanaNessuna valutazione finora
- Case Report Rehabilitation Program in A Patient With Tibial Condyle FractureDocumento26 pagineCase Report Rehabilitation Program in A Patient With Tibial Condyle FractureNatalia LoredanaNessuna valutazione finora
- Original Paper: Lumbar Disk Herniations - Clinical Status, Diagnosis, Imaging, Surgical Treatment and Global OutcomeDocumento6 pagineOriginal Paper: Lumbar Disk Herniations - Clinical Status, Diagnosis, Imaging, Surgical Treatment and Global Outcomeasep budiyantoNessuna valutazione finora
- Case Report Rehabilitation Program in A Patient With Fracture of The Distal FemurDocumento26 pagineCase Report Rehabilitation Program in A Patient With Fracture of The Distal FemurNatalia LoredanaNessuna valutazione finora
- Research Article: Correlation Between TMD and Cervical Spine Pain and Mobility: Is The Whole Body Balance TMJ Related?Documento8 pagineResearch Article: Correlation Between TMD and Cervical Spine Pain and Mobility: Is The Whole Body Balance TMJ Related?gloriagaskNessuna valutazione finora
- Comparison of Effect of Hip Joint Mobilization and Hip Joint Muscle Strengthening Exercises With Knee Osteoarthritis A. Tanvi, R. Amrita, R. Deepak, P. Kopal Srji Vol 3-Issue 1 Year 2014Documento13 pagineComparison of Effect of Hip Joint Mobilization and Hip Joint Muscle Strengthening Exercises With Knee Osteoarthritis A. Tanvi, R. Amrita, R. Deepak, P. Kopal Srji Vol 3-Issue 1 Year 2014Dr. Krishna N. Sharma100% (1)
- Case Report: Rehabilitation Program in A Patient With Congenital Dysplasia and Subluxation of The HipDocumento26 pagineCase Report: Rehabilitation Program in A Patient With Congenital Dysplasia and Subluxation of The HipNatalia LoredanaNessuna valutazione finora
- 1601Documento6 pagine1601labsoneducationNessuna valutazione finora
- Journal Pre-Proof: ExploreDocumento43 pagineJournal Pre-Proof: ExploreLuís CorreiaNessuna valutazione finora
- Clinical Rehabilitation: Does Electrical Stimulation Reduce Spasticity After Stroke? A Randomized Controlled StudyDocumento9 pagineClinical Rehabilitation: Does Electrical Stimulation Reduce Spasticity After Stroke? A Randomized Controlled StudyArkar SoeNessuna valutazione finora
- Wt-Ifu-1 - 1-Id-En 15-03-2021Documento28 pagineWt-Ifu-1 - 1-Id-En 15-03-2021Miguel SuntaxiNessuna valutazione finora
- Rehab 3.1 - Stroke Rehabilitation (Dr. Chan) - KV PDFDocumento4 pagineRehab 3.1 - Stroke Rehabilitation (Dr. Chan) - KV PDFCzara DyNessuna valutazione finora
- Facial PalsyDocumento7 pagineFacial PalsyPedro FonsecaNessuna valutazione finora
- Manual Do Estimulador Neuromuscular - Drager TofscanDocumento28 pagineManual Do Estimulador Neuromuscular - Drager TofscanRenato NascimentoNessuna valutazione finora
- Electrotherapy 2 Oral ExamDocumento7 pagineElectrotherapy 2 Oral ExamRody SaifNessuna valutazione finora
- Operating Manual For TENSmed 911 & 931 by ENRAF NONIUSDocumento39 pagineOperating Manual For TENSmed 911 & 931 by ENRAF NONIUSJAY2222QNessuna valutazione finora
- DocxDocumento4 pagineDocxKimNessuna valutazione finora
- Medical Equipment Business PlanDocumento53 pagineMedical Equipment Business PlanJemimah Mejia100% (3)
- Open Sim Tutorial 2Documento8 pagineOpen Sim Tutorial 2Mohd Khairul Ikhwan AhmadNessuna valutazione finora
- Motor Impairments Following StrokeDocumento31 pagineMotor Impairments Following StrokeFrancess LeveauNessuna valutazione finora
- DR - Azad.enraf - Sonopuls 490.user ManualeDocumento57 pagineDR - Azad.enraf - Sonopuls 490.user ManualeMohamed Bin ZainNessuna valutazione finora
- Chronic Electrical Nerve Stimulation As A Therapeutic Intervention For Peripheral Nerve RepairDocumento6 pagineChronic Electrical Nerve Stimulation As A Therapeutic Intervention For Peripheral Nerve RepaircontremonicaNessuna valutazione finora
- Electrotherapy, Laser, and Ultrasound PDFDocumento148 pagineElectrotherapy, Laser, and Ultrasound PDFkazakomNessuna valutazione finora
- Urinary Incontinence Has Sesven TypesDocumento55 pagineUrinary Incontinence Has Sesven TypesDhonat Flash100% (1)
- Electro-Acupuncture - An Introduction and Its Use For Peripheral Facial ParalysisDocumento19 pagineElectro-Acupuncture - An Introduction and Its Use For Peripheral Facial ParalysiserwindorinaldoNessuna valutazione finora
- Radiofrequncy Ablation in Chronic Pain ManagementDocumento21 pagineRadiofrequncy Ablation in Chronic Pain Managementtdiddy41Nessuna valutazione finora
- Sample Journal Review PaperDocumento14 pagineSample Journal Review PaperWharren DañoNessuna valutazione finora
- Physical Agent For Cancer Survvors An Updated Literatured ReviewDocumento9 paginePhysical Agent For Cancer Survvors An Updated Literatured ReviewDeborah SalinasNessuna valutazione finora
- Passion For Motion: Tensmed P82 & S82Documento46 paginePassion For Motion: Tensmed P82 & S82Mintflex Physiotherapy100% (1)
- Electrotherapy Assignment: Topic: 1. Current and Its Types 2. Procedure of Stimulation of Biceps Brachii MuscleDocumento12 pagineElectrotherapy Assignment: Topic: 1. Current and Its Types 2. Procedure of Stimulation of Biceps Brachii MuscleApoorvNessuna valutazione finora
- Development of Wireless Microcontroller Based Functional Electronic Stimulation Device For Drop Foot CorrectionDocumento87 pagineDevelopment of Wireless Microcontroller Based Functional Electronic Stimulation Device For Drop Foot CorrectionBrown KiswagaNessuna valutazione finora
- Rehabilitation Strategies After Spinal Cord InjuryDocumento17 pagineRehabilitation Strategies After Spinal Cord Injuryhanna.oravecz1Nessuna valutazione finora
- Physiotherapy Rehabilitation For People With Spinal Cord InjuriesDocumento8 paginePhysiotherapy Rehabilitation For People With Spinal Cord InjuriesAna Corina LopezNessuna valutazione finora
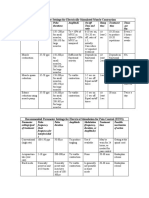
- Parameter Settings For Electrically Stimulated Muscle ContractionDocumento3 pagineParameter Settings For Electrically Stimulated Muscle Contractionpallen100% (5)
- Assessment of Neuroplasticity With Strength Training: Perspective For ProgressDocumento12 pagineAssessment of Neuroplasticity With Strength Training: Perspective For ProgressAgustin LopezNessuna valutazione finora
- Occupational Therapy Toolbox Study GuideDocumento44 pagineOccupational Therapy Toolbox Study GuideKristian ShumateNessuna valutazione finora
- Electrode Placement enDocumento40 pagineElectrode Placement enRichard HarrisNessuna valutazione finora
- Libble EuDocumento32 pagineLibble EuIvan AzenicNessuna valutazione finora
- HandbikeDocumento10 pagineHandbikeLely JuniariNessuna valutazione finora