Potrebbero piacerti anche
- Decision Process Quality ManagementDocumento144 pagineDecision Process Quality ManagementMark Levinsky100% (3)
- FDA 2008 D 0096 0032 - ContentDocumento10 pagineFDA 2008 D 0096 0032 - ContentAbdullah KamelNessuna valutazione finora
- Microbiological Safety of Mayonnaise, Salad Dressings, and Sauces Produced in The United States: A ReviewDocumento10 pagineMicrobiological Safety of Mayonnaise, Salad Dressings, and Sauces Produced in The United States: A ReviewAbdullah KamelNessuna valutazione finora
- SE Risk Assess Annex G Oct2005 PDFDocumento83 pagineSE Risk Assess Annex G Oct2005 PDFAbdullah KamelNessuna valutazione finora
- AA - Faguidelinespatient PDFDocumento36 pagineAA - Faguidelinespatient PDFAna Carolina TerrazzanNessuna valutazione finora
- GulfCooperationCouncilDraftsFoodGradeSaltStandardDocumento14 pagineGulfCooperationCouncilDraftsFoodGradeSaltStandardAbdullah KamelNessuna valutazione finora
- Statistical Process Control Tutorial Guide 010207Documento25 pagineStatistical Process Control Tutorial Guide 010207Revathi ChellamNessuna valutazione finora
- Microbiology Audit Guidance EbookDocumento23 pagineMicrobiology Audit Guidance EbookArmando Saldaña100% (1)
- Audit Scheme Reference Chart 2018 UpdateDocumento6 pagineAudit Scheme Reference Chart 2018 UpdateAquino Sianipar0% (1)
- Handbook of Food Spoilage YeastsDocumento23 pagineHandbook of Food Spoilage YeastsAdri De UdokNessuna valutazione finora
- Requirements For The FSSC 22000 V5 Upgrade ProcessDocumento3 pagineRequirements For The FSSC 22000 V5 Upgrade Processfiqrans100% (2)
- RAPasturized Liquid EggsDocumento109 pagineRAPasturized Liquid EggsAbdullah KamelNessuna valutazione finora
- FSSC 22000 Scheme Requirements: Detailed Changes Between V4 and V4.1Documento30 pagineFSSC 22000 Scheme Requirements: Detailed Changes Between V4 and V4.1mayaNessuna valutazione finora
- FSSC 22000 v4 To v4.1 Comparison Final Sep 2017Documento7 pagineFSSC 22000 v4 To v4.1 Comparison Final Sep 2017Abdullah KamelNessuna valutazione finora
- Materials Safety Data Sheet RENCO Annatto Food Colour (Hazardous)Documento3 pagineMaterials Safety Data Sheet RENCO Annatto Food Colour (Hazardous)Abdullah KamelNessuna valutazione finora
- Carotene Beta ScienceLabDocumento5 pagineCarotene Beta ScienceLabAbdullah KamelNessuna valutazione finora
- Juice Processing en (Small) PDFDocumento8 pagineJuice Processing en (Small) PDFAbdullah KamelNessuna valutazione finora
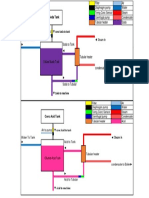
- Conc Soda TankDocumento1 paginaConc Soda TankAbdullah KamelNessuna valutazione finora
- Manual Fruits Veg 25 05 2016 PDFDocumento60 pagineManual Fruits Veg 25 05 2016 PDFShashikant DrShashikant BagadeNessuna valutazione finora
- JBT White Paper Filling Glass and Plastic BottlesDocumento8 pagineJBT White Paper Filling Glass and Plastic BottlesAbdullah KamelNessuna valutazione finora
- Juice Processing en (Small) PDFDocumento8 pagineJuice Processing en (Small) PDFAbdullah KamelNessuna valutazione finora
- Testing For EnzymesDocumento2 pagineTesting For EnzymesEmad AliNessuna valutazione finora
- 159 BulkMilkHaulerStudyGuideDocumento15 pagine159 BulkMilkHaulerStudyGuideAbdullah KamelNessuna valutazione finora
- Hot Fill PackagingDocumento15 pagineHot Fill PackagingSomasundaram Yamaraja100% (1)
- BPR Case HoneywellDocumento15 pagineBPR Case Honeywellravi5dipuNessuna valutazione finora
- Long Life ProductsDocumento228 pagineLong Life ProductsAbdullah KamelNessuna valutazione finora
- The Flemish Frozen-Vegetable Industry As An Example of Cluster AnalysisDocumento26 pagineThe Flemish Frozen-Vegetable Industry As An Example of Cluster AnalysisAbdullah KamelNessuna valutazione finora
- Six Sigma Metrics Existing Metrics Yield Scrap Rework ? ? ? ?Documento3 pagineSix Sigma Metrics Existing Metrics Yield Scrap Rework ? ? ? ?Mohammed KassemNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Chapter 3 Microbiology - 1443341834128Documento21 pagineChapter 3 Microbiology - 1443341834128Akil DhoniNessuna valutazione finora
- Characteristics of Well-Nourished Person With Optimum NutritionDocumento47 pagineCharacteristics of Well-Nourished Person With Optimum NutritionKaren Angela Torrecampo PelagioNessuna valutazione finora
- Pregnant WomenDocumento3 paginePregnant WomenmimiyuhhNessuna valutazione finora
- Normas DRISDocumento19 pagineNormas DRISRoger De Jesus Urrea LopezNessuna valutazione finora
- Soil Test Report Guide for FarmersDocumento6 pagineSoil Test Report Guide for FarmersHerbertNessuna valutazione finora
- Nderstanding Normal and Clinical Nutrition 9th Edition Rolfes Test BankDocumento35 pagineNderstanding Normal and Clinical Nutrition 9th Edition Rolfes Test Bankescout.stoopvr5nbf100% (24)
- New (Oumh1303) Breakfast Is The Most Important Meal of The DayDocumento6 pagineNew (Oumh1303) Breakfast Is The Most Important Meal of The DayjeckNessuna valutazione finora
- Dokumen KSKV HSK 101 Fundamental of Culinary ArtsDocumento13 pagineDokumen KSKV HSK 101 Fundamental of Culinary ArtsLee Yoke HanNessuna valutazione finora
- Neu Kam 2011Documento8 pagineNeu Kam 2011Jimena Caviedes DiepNessuna valutazione finora
- 7.1 Nutrition and Diet QP Olevel Cie BiologyDocumento22 pagine7.1 Nutrition and Diet QP Olevel Cie BiologyLaeeqNessuna valutazione finora
- 2.food and Its Components-Notes-2Documento2 pagine2.food and Its Components-Notes-2mohaddisaNessuna valutazione finora
- Nutrition ScienceDocumento24 pagineNutrition ScienceNihal BilalNessuna valutazione finora
- Recommended Dietary Allowances (Rda)Documento2 pagineRecommended Dietary Allowances (Rda)berrystrawberyNessuna valutazione finora
- Breast Milk CompositionDocumento2 pagineBreast Milk CompositionAisyah AzaniNessuna valutazione finora
- Good Habits and Healthy FoodDocumento13 pagineGood Habits and Healthy FoodJosé RosadoNessuna valutazione finora
- Food Technology PDFDocumento28 pagineFood Technology PDFMin ChongNessuna valutazione finora
- 13 Best Brain Foods Before ExamsDocumento3 pagine13 Best Brain Foods Before ExamsVidya NairNessuna valutazione finora
- The Leangains Encyclopedia Volume 1Documento106 pagineThe Leangains Encyclopedia Volume 1Dornilda Jovino De Almeida Aimbaré De Tucunduvá86% (7)
- Topic 1 The Chemistry of Life Unit One Molecules For LifeDocumento26 pagineTopic 1 The Chemistry of Life Unit One Molecules For LifekhotsoNessuna valutazione finora
- Handbook of Clinical Nutrition, 4th EditionDocumento644 pagineHandbook of Clinical Nutrition, 4th EditionLovely Rose83% (6)
- Batch sterilization methods and designDocumento28 pagineBatch sterilization methods and designPratibha PatilNessuna valutazione finora
- Specialist In Performance Nutrition GuideDocumento24 pagineSpecialist In Performance Nutrition GuidekalikNessuna valutazione finora
- The Perfect Keto Food ListDocumento57 pagineThe Perfect Keto Food Listpantera neagrăNessuna valutazione finora
- The Medicinal Chef Eat Your Way To Better HealthDocumento303 pagineThe Medicinal Chef Eat Your Way To Better HealthRogleva Roska100% (4)
- Food Science Dissertation IdeasDocumento6 pagineFood Science Dissertation IdeasWritingPaperServicesUK100% (1)
- Mapeh 7 Mapeh 7: (Health/Week 4)Documento17 pagineMapeh 7 Mapeh 7: (Health/Week 4)Elvin LlamesNessuna valutazione finora
- Modul 2.2Documento14 pagineModul 2.2sadyehNessuna valutazione finora
- Healthy Chicken Soup RecipeDocumento4 pagineHealthy Chicken Soup RecipeArishaNessuna valutazione finora
- Bodyboss - Superfood PDFDocumento280 pagineBodyboss - Superfood PDFWani Saparman85% (13)
- Fermentation Industry and Industrial AlcoholDocumento47 pagineFermentation Industry and Industrial AlcoholSOCRATESNessuna valutazione finora