Potrebbero piacerti anche
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Conflict ManagementDocumento4 pagineConflict ManagementSrimant DashNessuna valutazione finora
- Full BookDocumento152 pagineFull BookJezza WilsonNessuna valutazione finora
- UPSC Combined Mecical Services Examination 2012Documento7 pagineUPSC Combined Mecical Services Examination 2012TrcStaffNessuna valutazione finora
- Case 1 Hemiplegia With AphasiaDocumento8 pagineCase 1 Hemiplegia With Aphasialycan007Nessuna valutazione finora
- Femto Laser in OphthalmologyDocumento11 pagineFemto Laser in Ophthalmologylycan007Nessuna valutazione finora
- AIIMS May 2010Documento37 pagineAIIMS May 2010naveenmunNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- OVERVIEW Rapid Sequence Intubation (RSI) Is An Airway Management Technique That ProducesDocumento7 pagineOVERVIEW Rapid Sequence Intubation (RSI) Is An Airway Management Technique That ProducesOkami PNessuna valutazione finora
- Sanofi Aventis Vaccines Supply Chain ProcessDocumento21 pagineSanofi Aventis Vaccines Supply Chain ProcessarnaqviNessuna valutazione finora
- Schizencephaly A Review of 734 Cases PDFDocumento20 pagineSchizencephaly A Review of 734 Cases PDFDeglenNessuna valutazione finora
- AnophthalmiaDocumento6 pagineAnophthalmialeny zabidiNessuna valutazione finora
- Hospital MarketingDocumento39 pagineHospital Marketingdivyaky100% (1)
- Topics On Prosthetics & Orthotics - PDF CreDocumento4 pagineTopics On Prosthetics & Orthotics - PDF CreSuprit MahakudNessuna valutazione finora
- UHC Vision Plan SummaryDocumento2 pagineUHC Vision Plan SummaryJanet Zimmerman McNicholNessuna valutazione finora
- Low Cobalt Diet For Dyshidrotic Eczema PatientsDocumento5 pagineLow Cobalt Diet For Dyshidrotic Eczema PatientsMaulidianaIndahNessuna valutazione finora
- StuffDocumento4.804 pagineStuffSonder LegariNessuna valutazione finora
- Inhaled Anesthesia For BirdsDocumento18 pagineInhaled Anesthesia For BirdsBianca PaludetoNessuna valutazione finora
- Intro To Orthopedic Emergencies - RCSI Orthopaedic Emergencies - MK1Documento65 pagineIntro To Orthopedic Emergencies - RCSI Orthopaedic Emergencies - MK1kylieverNessuna valutazione finora
- TeratomaDocumento17 pagineTeratomaAndri Feisal NasutionNessuna valutazione finora
- NFDN 2005 Report On Progress PortfolioDocumento2 pagineNFDN 2005 Report On Progress Portfolioapi-329794748Nessuna valutazione finora
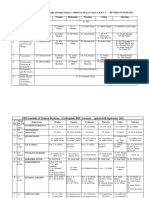
- Revised Schedule of BHU SSH OPD (Soft Copy) 2021Documento7 pagineRevised Schedule of BHU SSH OPD (Soft Copy) 2021rajubhagatssmNessuna valutazione finora
- Patient Queue Management SolutionDocumento34 paginePatient Queue Management Solutionmunish rattiNessuna valutazione finora
- GBD Lancet Paper 2 Dec 2012Documento27 pagineGBD Lancet Paper 2 Dec 2012lawrencehaddadNessuna valutazione finora
- DR - Prabhakar Patwardhan Samiti RugnalayaDocumento18 pagineDR - Prabhakar Patwardhan Samiti RugnalayaGajendra NikaleNessuna valutazione finora
- Rogers Textbook of Pediatric Intensive Care Fifth EditionDocumento61 pagineRogers Textbook of Pediatric Intensive Care Fifth Editiondanny.johnson566100% (40)
- Knowledge, Attitudes and Practices of The Medical Personnel Regarding Atopic Dermatitis in Yaoundé, CameroonDocumento7 pagineKnowledge, Attitudes and Practices of The Medical Personnel Regarding Atopic Dermatitis in Yaoundé, CameroonNadira Juanti PratiwiNessuna valutazione finora
- Nickel Titanium Rotary Instruments Making The Right Choice Jan 2012Documento6 pagineNickel Titanium Rotary Instruments Making The Right Choice Jan 2012Muchlis fauziNessuna valutazione finora
- MEMORANDUM OF AGREEMENT (Dentist)Documento2 pagineMEMORANDUM OF AGREEMENT (Dentist)thirdyjaoNessuna valutazione finora
- Introduction To Healthcare Quality Management-Examples From Hospitals in TaiwanDocumento4 pagineIntroduction To Healthcare Quality Management-Examples From Hospitals in TaiwanNai-Wen KuoNessuna valutazione finora
- Accident Investigation ProtocolsDocumento14 pagineAccident Investigation ProtocolsgilbertwildNessuna valutazione finora
- PRC Forms Bicol University COllege of Nursing, Legazpi CityDocumento5 paginePRC Forms Bicol University COllege of Nursing, Legazpi CityekagaliasNessuna valutazione finora
- Madhya Pradesh Ayurvigyan Parishad Adhiniyam 1987Documento12 pagineMadhya Pradesh Ayurvigyan Parishad Adhiniyam 1987Latest Laws TeamNessuna valutazione finora
- A ENT Fellowship For An Internation Resident - (Archive) - Student Doctor Network ForumsDocumento5 pagineA ENT Fellowship For An Internation Resident - (Archive) - Student Doctor Network ForumsAbhishek Kumar RamadhinNessuna valutazione finora
- Charateristics of NewbornDocumento3 pagineCharateristics of NewbornRagupathyRamanjuluNessuna valutazione finora
- Renal Calyceal MicrolithiasisDocumento3 pagineRenal Calyceal MicrolithiasisVic L. AmecaNessuna valutazione finora
- Cerebral PalsyDocumento31 pagineCerebral PalsyYunita Amilia0% (1)
- Gastrointestinal Bleeding in Infants and Children AAPDocumento16 pagineGastrointestinal Bleeding in Infants and Children AAPDina MarselinaNessuna valutazione finora