1
Internal medicine lec #4 part 1 Bronchial Asthma
19-3-2012
Dr. who gave this lecture is Basheer Khassawneh, MD, FCCP Bronchial Asthma is a common disease Sometimes in "TIME" magazine they talk about things that are common health problems that affect the society worldwide and Bronchial Asthma once made it to the cover page! Asthma is becoming more and more common
What is Bronchial Asthma? Do you know anybody with Bronchial Asthma? >> It is usually common! Definition helps you understand the disease, so it is an airway inflammation, and it is chronic not transient and goes away Causing recurrent episodes of symptoms, and this is what you see of asthma >> recurrent episodes of: o Wheezing o Breathlessness o Chest tightness o Dry cough o Cough particularly at night Symptoms are worse at night and/or in the early morning
Physiology of the disease: Variable airflow limitation, so they have a narrow airway that the air flow is limited And it is variable, so they have good\bad days, and good\bad hours
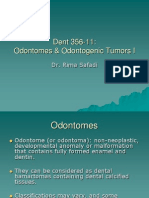
Reversibility in this obstruction becomes better spontaneously or with treatment "medication; bronchodilators for ex" Another property of asthma is Airway hyper-responsiveness to a variety of stimuli; which means when those patients are exposed to triggers, for example the wind outside and this cold air may cause people with asthma to start coughing and wheezing, dust, or strong smell The Scope of the Problem USA: -Affects 14 -15 million people, and it is a large number of people who have asthma -6% of children under the age of 18 years have asthma there, so it is also common in children, if you take a class or school 6% of the students would have true asthma and take medication for it -Inner city children have highest rates, so urbanized areas have more asthma than ruler areas -So we expect to see more asthma in more urbanized society, Amman, middle of Irbid, and Zarqa for example -Rates higher among females -In America rates higher among blacks, the Dr. doesn't think that here in Jordan <3 we have a huge ethnic diversity to judge! Family Members With Asthma 35.1% Past History of Asthma 5.8% Friends/Cowor kers With Asthma 29.4%
None 23.0%
3
Experience With Asthma: Public Survey They ask people around some Qs such as: do you have asthma? Did you have asthma? Do you have a family member having asthma? Do you know somebody who has asthma? As you can see in the chart above most of people either knows someone with asthma or they have it themselves
How the disease happens? It is a multifactorial disease (such as many internal med diseases) so there is no single defect that tells why you do have or don't have asthma Genetics plays a role through atopy "allergy", another effect of genetics has to do with cytokine dysregulation, and cytokines that are produced in the airways will have problems, excessive or reduced cytokines will help to produce asthma Environmental factors; Allergens, viruses' interactions, diet for example introducing early allergenic diet to children especially infants can cause asthma so parents should be very careful about what to feed their children in their early ages, and smoking either passive or active "for example kids who stay beside their smoking father or mother are more prone to respiratory tract infections than the others"
What happens at the cellular level? It is complicated and that's why its treatment is tricky, you will find histamine, leukotrienes, and cytokines who work on the epithelial and endothelial and cause inflammation And we have cytokines that works on macrophages and smooth muscles and cause inflammation So it is a multi-pathway disease >> for example in kids with asthma if you give them a drug that works on leukotrienes such as multi leukast they 4
usually improve because leukotrienes usually play an important and predominant role in asthma, BUT in adults it is not as effective as in children!
-Up until early 90s they used to think of asthma as a mechanical disease even physicians, asthmatics would have bronchoconstriction all they need is bronchodilators -As they started to take biopsies from asthmatic patients they realized that asthma is more than a bronchoconstriction -A lot of the lining epithelium in asthmatic airways is destroyed, and there is mucus plugging, if you take a lung biopsy from people who die from sever asthmatic attack will find a lot of mucus plugging, and bronchodilators cannot improve them at all :\ -And we have thickening, and an increase of the smooth muscles of the airways -It is not just a simple bronchoconstriction\ bronchodilation it is more than that, there will be lots of inflammation and this reflects our treatment of asthma patients Consequence of Inflammation in Asthma: -How do all of these pathways work? People with asthma history if they had a stimulus (Antigens, virus, pollutants, occupational agent) it will cause inflammation this inflammation might be acute episode >> 5
either goes away by itself or cause hyper-responsiveness and inflammation {the patient will have bronchoconstriction and cough etc} -Most of the patients will go into the "Chronic inflammation phase" which will cause injury such as edema and injury to the endothelium etc; to this injury body does repair what we call remodeling "repair with recurrent damage" which is important in Asthma -How do we see this repair in Asthmatic? A patient comes for example at the age to 20, he doesn't take medication, so he will have recurrent asthma repair inflammation and so on >> at the age of 30 he comes and says Dr. I used to have just a simple bronchodilator once in two weeks, then after few years I started to have regular use, but now I go to the emergency room and they give me steroids needles! NOW in his case it is a progressive disease, BUT usually it is not a progressive disease it is stable! A mild patient stays mild moderate stays moderate and so on, when do you cross these borders? >> When you have remodeling -So when we have changes on the cellular level only it is important to enforce management on patients so the Dr. tells his patients that if you don't want to take the medication now its fine but this simple medication won't help you after 3 or 5 years! -So Chronic inflammation with no medication lots of repair and inflammation and remodeling >> will lead to permanently altered lung function If you take a look at the lung function of a male non-smoker:
-From the age of 20-80 it slowly decreases but if you look at the asthmatic it is a rapid decrease because of remodeling and destruction of the airways! (So they lose their lung function with time) -Another important issue for public knowledge is that people say Asthma can go away this is true in children more than in adults, and it depends on the onset of which if it is at the early age "below 5 yrs" there is higher chance that the child when he grow up he will grow out of Asthma! -BUT for adulthood asthma the later Asthma will start the less likely this will occur (for example someone had asthma at the age of 25-30 it is unlikely asthma will go away) -The common Arabic terminology of the Bronchial Asthma is "al- rabo" and when you tell someone that you have Rabo he will believe that it will never go away which is true most of the adults will stay at this chronic phase, some of them will regress and some of them will progress, but most go into this stable chronic phase! Risk Factors for Asthma: o Allergy/Atopy which if familial we said people with eczema, conjunctivitis, or rhinitis makes it more likely to develop asthma! o Family history of asthma/allergy, so a child with parents having asthma is more likely to develop asthma than a child with healthy family! o Perinatal exposure to tobacco smoke, as we said before the Dr. thinks it is a crime for the parents to smoke inside the house and cause passive smoking to their children, because carcinogens will settle on the carpet and things in the house! o Early viral respiratory tract infections o Low birth weight o Environmental pollution o Low socio-economic status 7
o Passive smoking Atopy and Asthma: - Asthmatics are more atopic than non-asthmatics
Atopy (atopic syndrome) is a syndrome characterized by a tendency to be hyperallergic. A person with atopy typically presents with one or more of the following: eczema (atopic dermatitis), allergic rhinitis (hayfever), allergic conjunctivitis, or allergic asthma. Patients with atopy also have a tendency to have food allergies. Patients with atopy usually develop what is referred to as the allergic triad of symptoms, i.e., eczema (atopic dermatitis), hayfever (allergic rhinitis), and allergy-induced asthma (allergic asthma). They also have a tendency to have food allergies, and other symptoms characterized by their hyperallergic state. For example, eosinophilic esophagitis is found associated with atopic allergies. Atopic syndrome can be fatal for those that experience serious allergic reactions, such as anaphylaxis, brought on by reactions to food or environment. Wiki
-Some people come and ask for skin tests but they are usually not rewarding in asthmatics -They usually have multiple atopic reasons House dust mite for example and a number of things -House dust mite is the most common aer-allergen worldwide
-It lives in dust, it is everywhere, we are allergic to its feces we inhale it! {YUCK} -It is very hard to get rid of it, and very hard to avoid it Indoor Air Triggers: o Environmental tobacco smoke o Cockroaches o House dust mites - common o Animal dander - cats o Mold Outdoor Air Triggers: Here in Jordan <3 olives makes a problem because it is everywhere, and it produces strong air allergens o Particulate matter (air pollution) o Combustion products, maybe here in Jordan <3 it is not that much of a problem o Industrial emissions o Vehicle exhaust o Outdoor pollens >> Olive Additional Triggers: -1st problem as additional triggers for us as doctors are medications -Some patients with asthma they exacerbate by the use of aspirin o Viral upper respiratory infections o Exercise and hyperventilation o GERD
o Sinusitis and rhinitis o Diet o Cold air o Drugs o Aspirin, NSAID which are the most commonly used in Jordanian market and you as dentist want to give a patient a medication and you prescribe a NSAID for him and the exacerbate so you have to pay attention!, beta blockers Asthma Diagnosis: -It is usually diagnosed clinically by taking history and symptoms of the patient, as we said before they would have the Syndrome of Asthma (go back and review them) Symptoms and Signs: o Variety of symptoms o wheeze o shortness of breath o chest tightness o cough Asthma symptoms tend to be: o Variable and intermittent o Worse at night, and early mornings o Provoked by triggers, strong smells, cold air etc
10
Additional Elements in History: Personal or family history of: o Asthma o Atopic condition: eczema, allergic rhinitis >> makes the case stronger to be asthmatic as well Physical Signs of Asthma: -They can be normal, especially if he came to you as a dentist During exacerbations: Wheezes! Differential Diagnoses: -COPD, Chronic obstructive pulmonary disease, which occurs in elderly, in smokers usually, so it can be very similar to asthma -Acid reflux, they would have recurrent cough -Post nasal drip, usually with cough early in the morning -And other things that can mimic asthma: o Cystic fibrosis o Tumor: Laryngeal, tracheal, lung o Bronchiectasis o Foreign body o Vocal cord dysfunction o Hyperventilation Diagnostic Tools: >> Peak flow monitoring, a small piece of plastic that measures the peak flow >> Pulmonary function testing (spirometry), asthmatic patient who has an obstructive defect "pattern" they would 11
have: FEV1/FVC < 70% and the Forced Vital Capacity will decrease, and less FVC in 1 sec "decreased FVC1" -And they have reversibility >> which means when we give them a bronchodilator in the clinic and I test them again they would be better and with better airflow -FEV1 increases by 15% after inhalation of a rapid-acting beta-2-agonist Asthma Management: Goals of management nowadays are better: No (or minimal) daytime symptoms No limitations of activity No nocturnal symptoms No (or minimal) need for rescue medication Normal lung function No exacerbations
>> This is almost a normal person and this is achievable by medications Levels of Asthma Control: Not that much important :\ BUT take a look next page
12
Characteristic
Partly controlled (Any present in any (All of the following) week) Controlled None ( 2/ week) None > 2 / week Any
Uncontrolled
Daytime symptoms Limitations of activities Nocturnal symptoms / awakening Need for rescue / reliever treatment Lung function (PEF or FEV1)
None
Any
3 or more features of partly controlled asthma present in any week
None ( 2 / week)
> 2 / week
Normal
< 80% predicted or personal best (if known) on any day 1 / year 1 in any week
Exacerbation
None
-Doctors should believe that there is no current cure for asthma, but most important to know that if you give them medications "symptoms wide" they can live a normal life ^^: -While the doctor was preparing for the lecture he opened google pix and searched Bronchial asthma and the most common thing that he found is ??? Someone holding an inhaler! >>> So inhalers are stigma for Asthma! <<< Q: why some people have mild, moderate and severe? A: Asthma is just like a pyramid the top is severe and the bottom is mild and people can have any of which! Most of the time people stay wherever they are but sometimes they can get worse :\
-So most of the people stick at the level they are at! And if they are not treated they can cross the borders and get worse 13
-So we said Asthma is an inflammation so you should give antiinflammatory drugs and the best one is Inhaled glucocorticosteroids; because it is locally delivered to the site of the disease with minimal systemic effect -Leukotriene modifiers, as we said a subset of patients benefit from that especially children -We have a new treatment which is: Anti-IgE , for people with atopic or allergic Asthma, very expensive -An old medication: Theophylline, less used these days -We use Systematic glucocorticosteroids, during exacerbations and patients who doesn't respond >>So the main treatment of Asthma is: inhaled corticosteroids<< And the mortality rate among patients who don't take inhaled corticosteroids is much higher than those who take it! Reliever Medications Asthmatic patients have airway hyperresponsiveness and bronchospasm so we should give them bronchodilators as well The common bronchodilator is: Salbutamol Anticholinergics: Ipratropium, is also a good bronchodilator especially when combined with salbutamol -Steroids also can work as bronchodilators
14
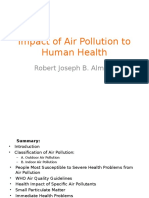
Those are the various types of inhalers that we have! And they have combination of medication within those inhalers, steroids and bronchodilators
15
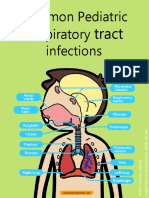
The figure above illustrates the step therapy for asthma It is a traditional slide for asthma patients everywhere you go you will find it Although we don't follow these rules, but as you can see the general concepts are important For example all patients should be well educated about their disease, and environmental control As you can see all patients take inhaled corticosteroids but with variable doses! Asthma Exacerbations Asthma during exacerbations is similar to regular asthma; let's look to asthma as camping fire you just put water on it to stop it what if you have a big fire in the whole wood! The same concept you bring water to stop it but in a larger scale! Asthma during exacerbation is similar to regular asthma, for example instead of inhaled CS we give systemic CS Instead of 2-agonists every 6 hours I give it every 4 hours and so They may be treated in the hospital! For example if you had a patient in your clinic and he had asthmatic attack you give him O2 (the amount doesn't really matter) followed by CS >> if they had good response that is good if not you give them systemic CS and then they go to the hospital!
16
There is an article in the magazine dentistry and medicine the Dr. advice us to look at it! it is about increased risk of caries in asthma patients and -Reduced salivary flow -Oral mucosal changes -Gingivitis -Orofacial abnormalities Increased upper anterior and total anterior facial height Higher palatal vaults Greater overjets Higher prevalence of posterior crossbites So there is an association between asthma and dental diseases! You should be aware if the patient has allergy to any component and if the local anesthetic is not good for him! As we said the attacks comes early in the morning so we tell them to go to the dentists in the afternoon! Take your medication before you go! Simple things make a big difference in management Qs? Dr. answered some Qs but they where general and he answered in general as well Dr. said Qs comes from the slides )( ..
17
Internal medicine lec #4 part 2 Community Acquired Pneumonia -Dr. who gave this lec is Shaher M. Samrah, MBBS, FCCP -Types of pneumonia: Community Acquired Pneumonia (CAP) Hospital Acquired Pneumonia Pneumonia in Immune-compromised Host
19-3-2012
Pneumonia in Patients with HIV >> which is considered a special type of pneumonia
-What we are concerned about is CAP Epidemiology -The sixth leading cause of death -The most common infectious cause of death Mortality < 1% in the outpatient setting will die -But the mortality increases according to the severity; 5-12% for patients requiring hospital admission and 22-50% for patients requiring ICU admission Microbiology We think of a variety of bacterial and viral pathogens, but CAP most commonly caused by bacteria Streptococcus pneumoniae is the most common organism In sever dental caries patients with bad oral hygiene and lots of cavities they would have anaerobic infections other than Streptococcus pneumoniae 18
Take a look at this list of pneumonias:
Alcoholism Streptococcus pneumoniae, oral anaerobes, Klebsiella pneumoniae, Acinetobacter species, Mycobacterium tuberculosis Haemophilus influenzae, Pseudomonas aeruginosa, Legionella species, S. pneumoniae, Moraxella catarrhalis, Chlamydophila pneumoniae Gram-negative enteric pathogens, oral anaerobes CA-MRSA, oral anaerobes, endemic fungal pneumonia, M. tuberculosis, atypical mycobacteria Histoplasma capsulatum
COPD and/or smoking
Aspiration Lung abscess
Exposure to bat or bird droppings Exposure to birds Exposure to rabbits Exposure to farm animals or parturient cats Influenza active in community
Chlamydophila psittaci (if poultry: avian influenza) Francisella tularensis Coxiella burnetti (Q fever)
Influenza, S. pneumoniae, Staphylococcus aureus, H. influenzae Bordetella pertussis
Cough >2 weeks with whoop or posttussive vomiting Structural lung disease (eg, bronchiectasis) Injection drug use Endobronchial obstruction In context of bioterrorism
Pseudomonas aeruginosa, Burkholderia cepacia, S. aureus S. aureus, anaerobes, M. tuberculosis, S. pneumoniae Anaerobes, S. pneumoniae, H. influenzae, S. aureus Bacillus anthracis (anthrax), Yersinia pestis (plague), Francisella tularensis (tularemia)
Alcoholism, Aspiration, Lung abscess all of which you can see anaerobic organisms in the list! So not everyone with CAP has streptococcal infection, but you have to think about it because it is the most common microorganism 19
And you should think of the risk factor that is most likely to cause the disease! Previously they used to say that there is what we call typical and atypical pneumonia but they don't use it anymore because and the might go inside each other's classes and in the end the treatment is the same, because as well at least 10-40% Co-infection with one pathogen of the list Diagnostic Approach to CAP Clinical Evaluation >> we start with History we ask about symptoms, fever, chills, and so on Physical exam Simple laboratory tests Radiological Evaluation Chest X-Ray CT chest Microbiological studies Clinical Evaluation: (Symptoms) 90% patients will have cough regardless productive or dry Purulent sputum Dyspnea Pleuritic chest pain Fever and chills Physical Signs: Vital signs: Tachycardia, tachypnea, fever, hypotension Signs of consolidation: This means when the lung has an infection! Dullness, egophony, crepetations bronchial breath sounds, 66% 66% 50% 30-40%
Signs of pleural effusion: this means fluid around the lung 20
Stony dullness "Dr.s have a test by the finger they knock on the cavity or any place in the body you should hear resonance when you don't hear it they cavity is filled with something else fluid or so", diminished breath sound
Investigation: Depends whether it is an outpatient or inpatient We start with Routine tests performed on admission: Chest radiograph Complete blood count Urea, electrolytes and liver function tests, because there are microorganisms that produce liver dysfunction Oxygenation assessment: ABG You detect if the patient has hypoxia SaO2 <92% on admission How to detect pneumonia: pulse oximetry, or by ABG "arterial blood gas" features of severe pneumonia Radiological Evaluation By definition, Pneumonia requires the finding of infiltrate on chest radiograph The presence of infiltrate on CXR is the gold standard for diagnosing pneumonia Radiological findings: -Lobar infiltrate: One lobe or multi-lobar -Interstitial infiltrate, all of the lung infected 21
-Pleural effusion: Parapneumonic or empyema And they may have: -Lung abscess -So when a patient comes to you and you start detecting the dysfunction and see what the symptoms that he has are, cough, fever, and shortness of breath I ask for an X-ray and you will find lobar infiltrate -What other things that I can do to help me diagnose? Some people might ask for culture from this lung to see what is this microorganism?
This is pneumonia in the right upper lobe of the lung
Here we have the right lower lobe having more infection, but you feel bilateral infiltrate exist! >> Right lower + middle Lobes
22
Here we can see the infection in the right lower lobe but there is effusion as well! >> Pleural Effusion
Here we have infiltrate on the left lower lobe, but there is some sort of fluid level! So cavity with fluid >> Lung abscess Microbiologic Diagnosis: Some people ask for sputum for culture which is good but should not guide you through diagnosis! Because you have to start treatment before, according to the risk factor
23
So you don't have to wait for culture to start treatment unless you have moderate and severe cases and you want to make sure of the microorganism that is causing the infection! Microbial cause is not found in 2560% of cases You diagnosis Should be guided by: The severity of pneumonia Epidemiological risk factors The response to treatment So Sputum culture is not really needed! ~ 30% has unable to produce sputum Helps to broaden the empiric antibiotic therapy o Blood Culture sometimes it is recommended preferably before antibiotic treatment, so when you have a patient you take a blood culture from him before you start antibiotics to make sure that you are not treating a resistant microorganism o Pleural fluid if the patient had plural infusion! Gram stain and culture o And in some cases we make what we call Bronchoscopy (BAL, PB) , .. In rare infection and rare presentations, and risk cases for example when a patient comes and you suspect he has TB and you tell him to give you sputum which has a totally different treatment! Pneumonia is a systemic infection it is not local it reaches the blood! So you have to start antibiotics as soon as possible And at least order blood culture and it helps you later on
24
For example when an outpatient comes we treat him without blood nor sputum culture so it depends on the severity and sometimes we don't use chest X-ray Serology: Sometimes you take a urine sample and you find antigens in it! So this helps to guide diagnosis but it doesn't guide treatment So you always have to treat Legionella for example And it helps in screening and epidemiological studies, BUT we don't wait for those to come back to decide treatment ^^: The antibiotics that we use in CAP cover those other organisms, such as Legionella, Pneumococcal antigens so usually the antibiotic covers the microorganisms included in the disease And sometimes you have other signs such as Legionella causes liver dysfunction for example and they have hyponatremia so in this case to make sure that Legionella is the cause and to rule out other dysfunctions we order a urine test or serum test It takes 4-6 weeks to get the results Which is not recommended to wait that much! As we said you have to decide where to treat out\in patient, and if the patient need to be in ICU We have some things that help us decide but we don't use them all For example: Pneumonia Severity Index (PSI) CURB-65 Pneumonia Severity Index (PSI)
25
We have classes from 1-5, depends on the scores 1\2 >> outpatient 4\5 >> inpatients More than 5 >> they usually go to ICU Those are the scoring points:
26
It is COMPLICATED and we don't use it often So we go to the other thing which is CURB 65 It is a summary of the risk factors and when we see them we say this patient has severe pneumonia and this doesn't C Confusion U Urea > 7 mmol/l R Respiratory rate > 30/min B BP: Systolic < 90 mm Hg Diastolic < 60 mm Hg Hypotension, renal failure, and confused patient! 65 Age > 65 Years
The older the patient the more severe his case will be! So if the patient had the things above he has severe pneumonia And if the patient had end organs involvement we say he has sepsis, it became systemic so there is risk factors in severe pneumonia that are really scary and we should take of them Studies play a role here because of the need of knowing the effect of the risk factors on the severity of the disease Criteria for Severe CAP The slides say minor and major not necessary, you know what the things you should think about to decide admission to ICU or not Major Criteria >> Invasive mechanical ventilation Patient that needs invasive ventilation Where to put him? 27
If the patient had Septic shock requiring vasopressors whatever the cause is It is very difficult to treat him in the floor Minor Criteria >> Respiratory rate > 30/min PaO2 / FIO2 < 250 Multi-lobar infiltrates Confusion Uremia (BUN > 20 mg/dl) Neutropenia Thrombocytopenia Hypothermia "the same as fever it is a bad thing that means the patient is no longer having defense no white cells defense to produce fever" Patients with very low oxygenation or having bilateral lung abscess they are at high risk of getting worse you're always concerned whether they'll need more oxygen CAP Treatment: Microbiological DX unknown in up to 50% Initiate therapy within 8 hours ((patient with pneumonia >> antibiotics)) Always think about co-infection and X-rays How to decide what kind of treatment you want to use?? >> If the patient was previously healthy, and did not use antibiotics "Previously healthy + No antimicrobials within the previous 3 months" Simple Macrolide is enough for example: eryhthromycin, Clarithromycin, Azithromycin 28
>> "Comorbidities or antimicrobials within the previous 3 months" -Respiratory fluoroquinolone: levofloxacin --lactam + macrolide The later we have to use two antibiotics because the microorganism pneumonia has 30% increased resistant Macrolide are not enough for severe pneumonia we have to use other antibiotics Inpatient Treatment-Non ICU Same as we said: Respiratory fluoroquinolone Levofloxacin, Moxifloxacin, Gemifloxacin -lactam + Macrolide Ceftriaxone, Cefotaxime Dental pneumonia! In cases of aspiration and lung abscess pneumoniae where anaerobic infection Which are found in the mouth dental caries, decays A patient that is alcoholic and is always sleeping, with bad oral hygiene which is a risk factor for two things: dental pneumonia, and infective endocarditic What are the antibiotics used in this case? Clindamycin (first-line therapy) covers anaerobic only Amoxicillin-clavulanate Metronidazole + Amoxicillin/Penicillin G
29
We have vaccinations:
There is another thing which is Influenza virus Vaccine
In October or November to decrease mortality from such as infections And they are given to the staff as well
30
It takes time to heal ... 4 weeks to resolve depends on the severity it is a reversible disease Most common pneumonia caused by bacteria It is infectious At the end the Dr. showed a pic of a casino in Las Vegas why I don't kn! Sorry for any mistake .. ~ " " - - : : ( ) ...
Life is short try not to waste it unhappy
31
Potrebbero piacerti anche
- New Microsoft Office Word DocumentDocumento2 pagineNew Microsoft Office Word DocumentJustDen09Nessuna valutazione finora
- Surgery-Past Years QsDocumento10 pagineSurgery-Past Years QsGaYda'a Kana'anNessuna valutazione finora
- Pedo 4Documento59 paginePedo 4JustDen09100% (1)
- Odontomes & Odontogenic Tumors II (Slide 18+19)Documento39 pagineOdontomes & Odontogenic Tumors II (Slide 18+19)JustDen09Nessuna valutazione finora
- Oral Ulceration and Vesiculobullous Diseases and 2Documento107 pagineOral Ulceration and Vesiculobullous Diseases and 2JustDen09100% (1)
- Pedo 4Documento59 paginePedo 4JustDen09100% (1)
- Lab Vesiculobullous and Ulcer at Ions (Lab 5)Documento55 pagineLab Vesiculobullous and Ulcer at Ions (Lab 5)JustDen09100% (1)
- Odontomes & Odontogenic Tumors I (Slide 17)Documento32 pagineOdontomes & Odontogenic Tumors I (Slide 17)JustDen09Nessuna valutazione finora
- 3 - Odontomes & Odontogenic TumorsDocumento63 pagine3 - Odontomes & Odontogenic TumorsAnȜ'am Abu Ȝ'leonNessuna valutazione finora
- Lab Oral Infections (Lab 4)Documento67 pagineLab Oral Infections (Lab 4)JustDen09100% (1)
- Infections of The Oral Mucosa 1 (Slide 10 + 11)Documento65 pagineInfections of The Oral Mucosa 1 (Slide 10 + 11)JustDen09Nessuna valutazione finora
- Infections of The Oral Mucosa 2 (Slide 12 +13)Documento58 pagineInfections of The Oral Mucosa 2 (Slide 12 +13)JustDen09Nessuna valutazione finora
- Review of Cobalt Chrome Denture Design 97-2003Documento44 pagineReview of Cobalt Chrome Denture Design 97-2003JustDen09100% (3)
- Lec#5 Sleep Apnea, InternalDocumento21 pagineLec#5 Sleep Apnea, InternalJustDen09Nessuna valutazione finora
- Diseases of The Temporomandibular JointDocumento27 pagineDiseases of The Temporomandibular JointJustDen090% (1)
- Keratoses and Related Disorders of Oral Mucosa I (Slide 3)Documento46 pagineKeratoses and Related Disorders of Oral Mucosa I (Slide 3)JustDen09Nessuna valutazione finora
- Dia BetsDocumento17 pagineDia Betsمحمد ابوالمجدNessuna valutazione finora
- I M Lec #3Documento25 pagineI M Lec #3JustDen09Nessuna valutazione finora
- Keratoses and Related Disorders of Oral Mucosa II (Slide 4 + 5 + 6)Documento83 pagineKeratoses and Related Disorders of Oral Mucosa II (Slide 4 + 5 + 6)JustDen09Nessuna valutazione finora
- Endodontic QuizzesDocumento5 pagineEndodontic QuizzesJustDen0980% (5)
- Major and Minor ConnectorsDocumento32 pagineMajor and Minor ConnectorsJustDen09100% (1)
- Dent 356 Midtermgrades No NamesDocumento7 pagineDent 356 Midtermgrades No NamesJustDen09Nessuna valutazione finora
- Lab Oral Epithelial Tumors (Lab 3)Documento57 pagineLab Oral Epithelial Tumors (Lab 3)JustDen09100% (1)
- Hyperplastic and Related Disorders of OM 2 (Script # 2)Documento20 pagineHyperplastic and Related Disorders of OM 2 (Script # 2)JustDen09Nessuna valutazione finora
- ALL Oral Epithelial Tumors I and II and III (Slide 7+8+9)Documento103 pagineALL Oral Epithelial Tumors I and II and III (Slide 7+8+9)JustDen09Nessuna valutazione finora
- Dent 356 Long Syllabus 2012Documento6 pagineDent 356 Long Syllabus 2012JustDen09Nessuna valutazione finora
- Dent 355 Rima Huda Lab KeratosisDocumento57 pagineDent 355 Rima Huda Lab KeratosisHeba S RadaidehNessuna valutazione finora
- Introduction, Cont. (Script # 2)Documento11 pagineIntroduction, Cont. (Script # 2)JustDen09Nessuna valutazione finora
- BIOSTATISTICS#1Documento10 pagineBIOSTATISTICS#1Sanaa QasemNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- B. Councils Report 2021-22-2Documento26 pagineB. Councils Report 2021-22-2Divye GuptaNessuna valutazione finora
- Review of Literature on Asthma Definition, Types, Diagnosis and TreatmentsDocumento23 pagineReview of Literature on Asthma Definition, Types, Diagnosis and TreatmentsPurple Ivy GuarraNessuna valutazione finora
- Specific Indications in Clinical PracticeDocumento58 pagineSpecific Indications in Clinical PracticeOccult Librarian100% (5)
- Thesis LatestDocumento77 pagineThesis LatestRizkhanRicafortManaoisNessuna valutazione finora
- Sujok Therapy Points ChartDocumento2 pagineSujok Therapy Points ChartZubair Azhari KaipattaNessuna valutazione finora
- Community Diagnosis NCM 113 2Documento63 pagineCommunity Diagnosis NCM 113 2Jewenson SalvadorNessuna valutazione finora
- Greyson 2019Documento10 pagineGreyson 2019Ziha Zia Leonita FauziNessuna valutazione finora
- McqsDocumento6 pagineMcqsPinkymekala HasanparthyNessuna valutazione finora
- The Significance of Asthma FolDocumento7 pagineThe Significance of Asthma FolDedhy HartantoNessuna valutazione finora
- TREXA Website Update 2Documento2 pagineTREXA Website Update 2Mohammed Ramzy GhifariNessuna valutazione finora
- 1st Level and 2nd Level AssesmentDocumento3 pagine1st Level and 2nd Level AssesmentLeighvan PapasinNessuna valutazione finora
- Forced Expiration Exercises in Asthma and Their Effect On FEVDocumento3 pagineForced Expiration Exercises in Asthma and Their Effect On FEVdelphineNessuna valutazione finora
- Everything You Need To Know About AllergiesDocumento26 pagineEverything You Need To Know About AllergiesGiuliana FloresNessuna valutazione finora
- Health Impact of Air PollutionDocumento15 pagineHealth Impact of Air Pollutionapi-304969581Nessuna valutazione finora
- German Marine Agencies, Inc., Et Al. Petitioners, vs. Teodolah R. Caro, in Behalf of Her Husband Eduardo v. Caro, Respondent.Documento5 pagineGerman Marine Agencies, Inc., Et Al. Petitioners, vs. Teodolah R. Caro, in Behalf of Her Husband Eduardo v. Caro, Respondent.Francis Coronel Jr.Nessuna valutazione finora
- Other Health ImpairmentDocumento38 pagineOther Health ImpairmentCatherine DizonNessuna valutazione finora
- Australian Asthma Handbook - Asthma Score TableDocumento2 pagineAustralian Asthma Handbook - Asthma Score TableAminudin Aditya PamungkasNessuna valutazione finora
- Evaluation of Doctor's Knowledge, Attitude, Adherence To Clinical Practice Guideline-Gina 2011 - Recommendarions and Cost Associated With Asthma TreatmentDocumento47 pagineEvaluation of Doctor's Knowledge, Attitude, Adherence To Clinical Practice Guideline-Gina 2011 - Recommendarions and Cost Associated With Asthma TreatmentMuhammad IbnRaimyNessuna valutazione finora
- Journal 4 2020Documento11 pagineJournal 4 2020Iin Sakinah DewiNessuna valutazione finora
- Common Pediatric Respiratory InfectionsDocumento13 pagineCommon Pediatric Respiratory InfectionsAisha JailaniNessuna valutazione finora
- Reading: Task 1Documento9 pagineReading: Task 1123123Nessuna valutazione finora
- Asthma COPD and InhalersDocumento37 pagineAsthma COPD and InhalersDexter SiaNessuna valutazione finora
- Chronic Obstructive Pulmonary Disease (Lancet)Documento16 pagineChronic Obstructive Pulmonary Disease (Lancet)marcos gamboaNessuna valutazione finora
- Bronchial Asthma Diagnosis & TreatmentDocumento3 pagineBronchial Asthma Diagnosis & TreatmentHugh JacobsNessuna valutazione finora
- WP Contentuploads202305GINA 2023 Full Report 2023 WMS PDFDocumento246 pagineWP Contentuploads202305GINA 2023 Full Report 2023 WMS PDFJaquelin GarciaNessuna valutazione finora
- QUIZ ROUND-2 ASTHMA RAPID FIRE QUESTIONSDocumento58 pagineQUIZ ROUND-2 ASTHMA RAPID FIRE QUESTIONSSwati SharmaNessuna valutazione finora
- Drug ListDocumento18 pagineDrug ListMinh PhungNessuna valutazione finora
- Manual Emergency Revise EdditionDocumento264 pagineManual Emergency Revise Edditionshahidchaudhary100% (5)
- Male Birth Control Pill DiscoveryDocumento7 pagineMale Birth Control Pill DiscoveryJayson SolomonNessuna valutazione finora
- Asthma Case StudyDocumento4 pagineAsthma Case Studymp1757Nessuna valutazione finora