Potrebbero piacerti anche
- A Simple Guide To Urinary Stones, Diagnosis, Treatment And Related ConditionsDa EverandA Simple Guide To Urinary Stones, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Urinary System: Cytology, Histology, Cystoscopy, and RadiologyDa EverandUrinary System: Cytology, Histology, Cystoscopy, and RadiologyNessuna valutazione finora
- Urology MCQsDocumento13 pagineUrology MCQsRahmah Shah Bahai83% (6)
- Urology Quiz 10 MCQ AnswerDocumento2 pagineUrology Quiz 10 MCQ Answeruroquiz50% (2)
- Urology NotesDocumento8 pagineUrology NotesCzarinah Bacuado67% (3)
- Clinical UrologyDocumento98 pagineClinical Urologythapan87100% (2)
- Medical Facts and MCQ'S - Urology MCQDocumento15 pagineMedical Facts and MCQ'S - Urology MCQAhmed KassemNessuna valutazione finora
- Urology Essay QuestionsDocumento2 pagineUrology Essay QuestionsPeter AbikoyeNessuna valutazione finora
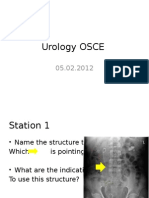
- Urology OSCE: Radiological AbnormalitiesDocumento9 pagineUrology OSCE: Radiological AbnormalitiesJihad Anad75% (4)
- Urology 90 Seconds - Buku 1Documento202 pagineUrology 90 Seconds - Buku 1Ari Alauddin100% (1)
- MCQ Uro1Documento1 paginaMCQ Uro1Kamal El-Ghorory67% (3)
- UrologyQuiz2 FollowupMCQ and AnswersDocumento1 paginaUrologyQuiz2 FollowupMCQ and AnswersUrologyQuizNessuna valutazione finora
- Genito-Urinary Tract 37Documento6 pagineGenito-Urinary Tract 37Hasan A AsFourNessuna valutazione finora
- Aua 2012 PDFDocumento39 pagineAua 2012 PDFMohsen100% (1)
- Urology Sample MCQ Exam eDocumento5 pagineUrology Sample MCQ Exam eDALIA100% (2)
- Urology DNB Old QuestionsDocumento8 pagineUrology DNB Old QuestionssjulurisNessuna valutazione finora
- UrologyQuiz8FollowupMCQ and AnswersDocumento2 pagineUrologyQuiz8FollowupMCQ and Answersuroquiz100% (2)
- Aua 2012Documento90 pagineAua 2012Tawfiq El-Far100% (5)
- UrologyQuiz6FollowupMCQ and AnswersDocumento2 pagineUrologyQuiz6FollowupMCQ and AnswersUrologyQuiz83% (6)
- Urology Grey ManualDocumento115 pagineUrology Grey ManualdmshossainNessuna valutazione finora
- Urology Quiz 9 MCQ AnswerDocumento2 pagineUrology Quiz 9 MCQ Answeruroquiz100% (2)
- Urology Residency Handbook 2018Documento64 pagineUrology Residency Handbook 2018Kshitij Kirane100% (2)
- Renal Notes Step 2ckDocumento34 pagineRenal Notes Step 2cksamreen100% (1)
- MCQDocumento24 pagineMCQHUSAMNessuna valutazione finora
- Urology Complete Qbank PDFDocumento58 pagineUrology Complete Qbank PDFPanda Panda100% (1)
- 2010 SaspDocumento115 pagine2010 Saspحسام أحمد عادلNessuna valutazione finora
- Benign Prostatic HypertrophyDocumento111 pagineBenign Prostatic HypertrophyOnkar SinghNessuna valutazione finora
- TOPIC NAME-GP Urology MCQsDocumento9 pagineTOPIC NAME-GP Urology MCQsAsif Newaz100% (1)
- Urology Quiz PDFDocumento7 pagineUrology Quiz PDFParsaant Singh100% (1)
- UrologyDocumento36 pagineUrologyakufahaba100% (2)
- Urology DossierDocumento166 pagineUrology DossierPeterNessuna valutazione finora
- 400L 2021 UROLOGY MCQsDocumento5 pagine400L 2021 UROLOGY MCQsApata OmotolaNessuna valutazione finora
- Quiz7 Follow-Up MCQS: (Answers Below!) MCQ: @urologyquizDocumento2 pagineQuiz7 Follow-Up MCQS: (Answers Below!) MCQ: @urologyquizUrologyQuizNessuna valutazione finora
- Dr. Anad's Guide to Urosepsis: Causes, Symptoms and TreatmentDocumento23 pagineDr. Anad's Guide to Urosepsis: Causes, Symptoms and TreatmentJihad Anad100% (1)
- Urology 2Documento57 pagineUrology 2Ostaz100% (1)
- Urology Smart PhrasesDocumento1 paginaUrology Smart PhrasesBrett FieldsNessuna valutazione finora
- Uro MCQDocumento12 pagineUro MCQLouisa Abigail D'Cruz100% (4)
- Exam Osce 3Documento37 pagineExam Osce 3momo100% (1)
- Answer For Urology MCQDocumento1 paginaAnswer For Urology MCQJihad AnadNessuna valutazione finora
- Urology Slides: DR - JihadDocumento4 pagineUrology Slides: DR - JihadJihad Anad100% (1)
- UrologyDocumento12 pagineUrologyThakoon Tts100% (1)
- Urological Emergency Presentations and ManagementDocumento83 pagineUrological Emergency Presentations and ManagementAlfred LiNessuna valutazione finora
- Recurrent urinary tract infections and staghorn calculusDocumento56 pagineRecurrent urinary tract infections and staghorn calculusHardiTariqHammaNessuna valutazione finora
- Urological History Taking FrameworkDocumento5 pagineUrological History Taking FrameworkahmadNessuna valutazione finora
- Urology Case Presentation - Scrotal Mass 1Documento20 pagineUrology Case Presentation - Scrotal Mass 1Hakimah K. Suhaimi100% (1)
- Urology MCQ Guide Hematuria Most Ominous SignDocumento16 pagineUrology MCQ Guide Hematuria Most Ominous SignChristian Jara80% (5)
- MCH UrologyDocumento20 pagineMCH UrologySholayMeiteiKangjamNessuna valutazione finora
- Chapter 02 Short Case On Parotid SwellingDocumento6 pagineChapter 02 Short Case On Parotid SwellingMonir Hossain Reza0% (1)
- Pujo / UpjoDocumento39 paginePujo / UpjoHafizur RashidNessuna valutazione finora
- NEET-SS Urology Mock Exam presents National-level Free MOCK EXAM on NEET-SS: UrologyDocumento59 pagineNEET-SS Urology Mock Exam presents National-level Free MOCK EXAM on NEET-SS: UrologyadiNessuna valutazione finora
- Pocket Manual On The Art of History TakingDocumento89 paginePocket Manual On The Art of History TakingAkwu Akwu100% (1)
- Prostatitis AUA 2017Documento29 pagineProstatitis AUA 2017Andres Felipe Cordoba AriasNessuna valutazione finora
- Nada's GI Path ReviewDocumento44 pagineNada's GI Path ReviewNada Much100% (2)
- Urology Course Covers Congenital AnomaliesDocumento236 pagineUrology Course Covers Congenital AnomaliesAlexandra BalanNessuna valutazione finora
- UROLOGYDocumento26 pagineUROLOGYgan choon huiNessuna valutazione finora
- 7 Liver - Spleen TraumaDocumento34 pagine7 Liver - Spleen Traumabagus75% (4)
- A System of Operative Surgery, Volume IV (of 4)Da EverandA System of Operative Surgery, Volume IV (of 4)Valutazione: 4 su 5 stelle4/5 (1)
- Arterial Blood Gas Interpretation – A case study approachDa EverandArterial Blood Gas Interpretation – A case study approachValutazione: 1 su 5 stelle1/5 (1)
- A Prospective Study On Therapeutic Management and Outcome Measures in Renal Failure PatientsDocumento5 pagineA Prospective Study On Therapeutic Management and Outcome Measures in Renal Failure Patientsvathsalya porankiNessuna valutazione finora
- Reimbursement Coding Guide Hemodialysis CathetersDocumento14 pagineReimbursement Coding Guide Hemodialysis CathetersLucy AndrianiNessuna valutazione finora
- CASE STUDY ON ACUTE Renal FailureDocumento38 pagineCASE STUDY ON ACUTE Renal FailureOdey Godwin100% (1)
- Abbreviations & Acronyms MeaningDocumento15 pagineAbbreviations & Acronyms MeaningNathaniel PulidoNessuna valutazione finora
- Kode Kombinasi Icd 10 Dan Icd 9 Indonesia Update 2019Documento11 pagineKode Kombinasi Icd 10 Dan Icd 9 Indonesia Update 2019[pml100% (1)
- Us 6913056Documento28 pagineUs 6913056roux76Nessuna valutazione finora
- Treatment of Chronic Kidney DiseaseDocumento12 pagineTreatment of Chronic Kidney Diseaseaty100% (1)
- Fin e 171 2014 PDFDocumento66 pagineFin e 171 2014 PDFRenugopalNessuna valutazione finora
- Chronic Kidney Disease NotesDocumento13 pagineChronic Kidney Disease NotesSwathi MathiazhaganNessuna valutazione finora
- Hemodialysis System: September 2012Documento23 pagineHemodialysis System: September 2012Hamed64Nessuna valutazione finora
- Acute Kidney InjuryDocumento34 pagineAcute Kidney Injury* mokhtar !!Nessuna valutazione finora
- KOD Final Year (M.B.B.S) - Survival GuideDocumento30 pagineKOD Final Year (M.B.B.S) - Survival GuideMubasharAbrarNessuna valutazione finora
- 2016 - Article - AbstractsForThe17thIPNACongres UrotomografiaDocumento219 pagine2016 - Article - AbstractsForThe17thIPNACongres UrotomografialeydyNessuna valutazione finora
- Hepatorenal Syndrome - UpToDateDocumento26 pagineHepatorenal Syndrome - UpToDateAssault AmphibiansNessuna valutazione finora
- 216093371Documento48 pagine216093371khuzaima933% (15)
- Physioloical Integrity Acute Biologic CrisisDocumento42 paginePhysioloical Integrity Acute Biologic CrisisJohn Paul M. TagapanNessuna valutazione finora
- Apport de Lhemodialyse Dans Linsuffisance Renale Aigue Obstructive: Benefices Et RisquesDocumento8 pagineApport de Lhemodialyse Dans Linsuffisance Renale Aigue Obstructive: Benefices Et RisquesIJAR JOURNALNessuna valutazione finora
- E000836 FullDocumento7 pagineE000836 Fullalejandro montesNessuna valutazione finora
- Bildiri 2021 - Orta Çağ İngiltere'Sinde Yargı Sisteminde Jüri Uygulamasının Kökeni Ve Kurumsallaşması Ss 51-60 - Halil YAVAŞDocumento450 pagineBildiri 2021 - Orta Çağ İngiltere'Sinde Yargı Sisteminde Jüri Uygulamasının Kökeni Ve Kurumsallaşması Ss 51-60 - Halil YAVAŞAnonymous zdK2MrNessuna valutazione finora
- Consultation 8Documento2 pagineConsultation 8api-28530178350% (6)
- Biomarkers in Kidney Disease PDFDocumento1.212 pagineBiomarkers in Kidney Disease PDFAndreea AdaNessuna valutazione finora
- Discussion 1 NPNDocumento53 pagineDiscussion 1 NPNFaith TambongNessuna valutazione finora
- 2018-089. NASKAH PUBLIKASI Elsi Nursyahdin MayaranaDocumento12 pagine2018-089. NASKAH PUBLIKASI Elsi Nursyahdin MayaranaElsi NursyahdinNessuna valutazione finora
- CKD Assessment and ManagementDocumento98 pagineCKD Assessment and ManagementDr Harihar KhanalNessuna valutazione finora
- Urinalysis ChecklistDocumento7 pagineUrinalysis ChecklistLana LocoNessuna valutazione finora
- Case Study CKD DM Type 2Documento7 pagineCase Study CKD DM Type 2Brian Cornel0% (3)
- Nursing exam covers hypertension, anemia, surgeryDocumento8 pagineNursing exam covers hypertension, anemia, surgeryBurhan uddin100% (2)
- CC Lab 6 TransesDocumento6 pagineCC Lab 6 TransesCiara PamonagNessuna valutazione finora
- Renal Disease and Neurology (2017)Documento22 pagineRenal Disease and Neurology (2017)mysticmdNessuna valutazione finora
- 08 Claim FormDocumento4 pagine08 Claim Formanurag1309Nessuna valutazione finora