Potrebbero piacerti anche
- General Biology 1 NOTES PDFDocumento18 pagineGeneral Biology 1 NOTES PDFRose Mendizabal82% (17)
- Toltec Body Healing EbookDocumento204 pagineToltec Body Healing EbookDanielle Grace100% (3)
- List of Anesthesia Library BooksDocumento3 pagineList of Anesthesia Library BooksSivaramakrishnan Dhamotharan100% (2)
- PacuDocumento24 paginePacuLamtioma GultomNessuna valutazione finora
- Respiratory Assessment GuidelinesDocumento1 paginaRespiratory Assessment GuidelinesAmeliaM100% (2)
- Gunshot WoundDocumento57 pagineGunshot Woundnecrophilia090407Nessuna valutazione finora
- Sodium Chloride Injection and Intravenous Infusion-PiDocumento4 pagineSodium Chloride Injection and Intravenous Infusion-PiNg Chee LunNessuna valutazione finora
- Learning and Memory 3rd Edition Gluck Test BankDocumento26 pagineLearning and Memory 3rd Edition Gluck Test Banklaurenhaynesnjqcdgotay100% (15)
- Bio Lab ReportDocumento7 pagineBio Lab Reportjoylee05Nessuna valutazione finora
- Anaesthesia RecordDocumento1 paginaAnaesthesia RecordАндрій ДанильцівNessuna valutazione finora
- Form 7389 Medical Record AnesthesiaDocumento3 pagineForm 7389 Medical Record Anesthesiasabbo morsNessuna valutazione finora
- 5-Hole 1/4 1 3/8 C-To-C: Anesthesia RecordDocumento10 pagine5-Hole 1/4 1 3/8 C-To-C: Anesthesia RecordMohammed100% (2)
- ICU One Pager NIPPVDocumento1 paginaICU One Pager NIPPVNicholas HelmstetterNessuna valutazione finora
- Agenda Bls-AclsDocumento2 pagineAgenda Bls-AclsespegehNessuna valutazione finora
- NeralDocumento9 pagineNeralmmNessuna valutazione finora
- AnesthesiaDocumento2 pagineAnesthesiaYuna WidjajaNessuna valutazione finora
- DPN Icu PDFDocumento1 paginaDPN Icu PDFharoonNessuna valutazione finora
- JD Respiratory TherapistDocumento3 pagineJD Respiratory TherapistLawrence MacaraegNessuna valutazione finora
- VentilatorWebinar1-Prof YasserDocumento28 pagineVentilatorWebinar1-Prof YasserShuaa AlabdulsalamNessuna valutazione finora
- Suez Canal University/ Faculty of Nursing (Medical Surgical Nursing/ Clinical Assessment Sheet 2 Year 2020/2021)Documento18 pagineSuez Canal University/ Faculty of Nursing (Medical Surgical Nursing/ Clinical Assessment Sheet 2 Year 2020/2021)طالب جامعة100% (1)
- Pediatric Assessment: General ImpressionDocumento2 paginePediatric Assessment: General ImpressionAghnia Nafila100% (1)
- Pediatric AnesthesiaDocumento6 paginePediatric AnesthesiaKeyien RadonesNessuna valutazione finora
- Introduction To Pediatric VentilationDocumento41 pagineIntroduction To Pediatric Ventilationedderj2585Nessuna valutazione finora
- Basic Mechanical Ventilation 2014Documento62 pagineBasic Mechanical Ventilation 2014dragon66Nessuna valutazione finora
- HANDOUTS-Non Invasive VentilationDocumento15 pagineHANDOUTS-Non Invasive VentilationKristine MangasepNessuna valutazione finora
- How To Treat: Septic ShockDocumento6 pagineHow To Treat: Septic ShockmeeandsoeNessuna valutazione finora
- Respiratory Therapist, NICU/ICUDocumento5 pagineRespiratory Therapist, NICU/ICUapi-77517256Nessuna valutazione finora
- Bsn-Rs-Careplan 2Documento9 pagineBsn-Rs-Careplan 2api-520841770Nessuna valutazione finora
- ACLS Class Packet PDFDocumento9 pagineACLS Class Packet PDFImam GultomNessuna valutazione finora
- An Easy Guide To Head To Toe Assessment Vrtis 12 2008 WebsiteDocumento6 pagineAn Easy Guide To Head To Toe Assessment Vrtis 12 2008 WebsiteGary Cochran100% (1)
- A B C D e AssessmentDocumento6 pagineA B C D e AssessmentANGELICA JANE FLORENDONessuna valutazione finora
- Medical Emergencies OMFSDocumento72 pagineMedical Emergencies OMFSkatnev100% (1)
- Location at Time of Fall (Ward, Clinic, Service, Etc.) : - Inpatient Outpatient Date of Fall: Time of Fall (Military)Documento5 pagineLocation at Time of Fall (Ward, Clinic, Service, Etc.) : - Inpatient Outpatient Date of Fall: Time of Fall (Military)Eduard RiparipNessuna valutazione finora
- Preparation-Surgical Area: Have To Operate Without ConsentDocumento5 paginePreparation-Surgical Area: Have To Operate Without ConsentJane Bautista100% (1)
- PRE ANAESTHETIC ASSESSMENT New 1Documento41 paginePRE ANAESTHETIC ASSESSMENT New 1lokeswara reddyNessuna valutazione finora
- 2020 Acls Megacode Testing Scenarios - 2Documento13 pagine2020 Acls Megacode Testing Scenarios - 2Dr. Saqib RazaNessuna valutazione finora
- Critical Care Skills Checklist: Personal InformationDocumento5 pagineCritical Care Skills Checklist: Personal InformationRin noharaNessuna valutazione finora
- Module 9 Mechanical Ventilation PDFDocumento46 pagineModule 9 Mechanical Ventilation PDFChabboo SutabrataNessuna valutazione finora
- Downtime Daily Nursing Assessment & Care Plan: 1 of 5 Date: TimeDocumento5 pagineDowntime Daily Nursing Assessment & Care Plan: 1 of 5 Date: TimerupaliNessuna valutazione finora
- Acls Seminar MeDocumento62 pagineAcls Seminar MeAbnet Wondimu100% (1)
- Patient History TemplateDocumento2 paginePatient History TemplateDr Shazana NazrinNessuna valutazione finora
- Pulmonary Function Testing1Documento51 paginePulmonary Function Testing1kusaarNessuna valutazione finora
- Chapter 5: Analyzing A Rhythm StripDocumento7 pagineChapter 5: Analyzing A Rhythm StriptellyNessuna valutazione finora
- Anesthesia ManualDocumento21 pagineAnesthesia ManualDocFrankNessuna valutazione finora
- Cardiac DrugsDocumento3 pagineCardiac DrugsRon WoodardNessuna valutazione finora
- 1008 1400 ACLS - StudyGuide Print PDFDocumento54 pagine1008 1400 ACLS - StudyGuide Print PDFWaqar HassanNessuna valutazione finora
- 17 Admission APP MED 001Documento8 pagine17 Admission APP MED 001HAMMYER ALROKHAMINessuna valutazione finora
- Cardiology Teaching PackageDocumento9 pagineCardiology Teaching PackageRicy SaiteNessuna valutazione finora
- Airway MXDocumento47 pagineAirway MXansuh22Nessuna valutazione finora
- Anesthesia RecordDocumento1 paginaAnesthesia Recordpcellaneous pc rentalsNessuna valutazione finora
- Cardiovascular Disorders 1Documento44 pagineCardiovascular Disorders 1Nader Smadi100% (1)
- BLS Study Guide 020620013Documento38 pagineBLS Study Guide 020620013R RatheeshNessuna valutazione finora
- Intravenous Anesthetic AgentsDocumento23 pagineIntravenous Anesthetic Agentsdrhiwaomer100% (7)
- Anaphylaxis With Angioedema: Section I: Scenario DemographicsDocumento7 pagineAnaphylaxis With Angioedema: Section I: Scenario DemographicsharasthaNessuna valutazione finora
- Anaphylaxis CEACCP 2004Documento3 pagineAnaphylaxis CEACCP 2004kuruppukarlNessuna valutazione finora
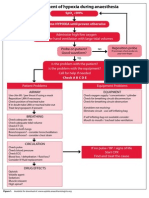
- Management of Hypoxia During AnaesthesiaDocumento5 pagineManagement of Hypoxia During AnaesthesiaNurhafizahImfista100% (1)
- 5 Shock PPT EnglishDocumento77 pagine5 Shock PPT EnglishKessi VikaneswariNessuna valutazione finora
- Antrim ED Handbook 2019Documento238 pagineAntrim ED Handbook 2019Chris Jardine LiNessuna valutazione finora
- Mechanical Ventilation Airway Pressure Release Ventilation Checklist Respiratory Therapy - 070420Documento3 pagineMechanical Ventilation Airway Pressure Release Ventilation Checklist Respiratory Therapy - 070420shubham2812Nessuna valutazione finora
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNessuna valutazione finora
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNessuna valutazione finora
- Lapsus Cardio v3Documento31 pagineLapsus Cardio v3Nurfitrianti ArfahNessuna valutazione finora
- Intern Survival Guide (UIC)Documento51 pagineIntern Survival Guide (UIC)medstick100% (1)
- ShockDocumento75 pagineShockaulianmediansyahNessuna valutazione finora
- Lecture Notes On Biophysics and Bioimaging 2009Documento128 pagineLecture Notes On Biophysics and Bioimaging 2009Anonymous 9rJe2lOskx100% (2)
- Semi-Detailed Lesson Plan in SCIENCE Grade 9Documento4 pagineSemi-Detailed Lesson Plan in SCIENCE Grade 9Sheryll Cayme SalindoNessuna valutazione finora
- Pathoma, Sketchy Pharm & Micro, B&B Video TimesDocumento52 paginePathoma, Sketchy Pharm & Micro, B&B Video TimesAlina PolancoNessuna valutazione finora
- Nitrogen CycleDocumento10 pagineNitrogen CyclebellaNessuna valutazione finora
- What Is Peritoneal DialysisDocumento34 pagineWhat Is Peritoneal DialysisKen MagallanesNessuna valutazione finora
- 07 Bibliography FormatDocumento14 pagine07 Bibliography FormatArjun KafleNessuna valutazione finora
- Cell 1981 Cech PDFDocumento10 pagineCell 1981 Cech PDFSpellkingNessuna valutazione finora
- AED (Automated External Defibrilation)Documento17 pagineAED (Automated External Defibrilation)Ari AsriniNessuna valutazione finora
- Weeks 3 - 8Documento32 pagineWeeks 3 - 8Stefan HutsonNessuna valutazione finora
- Chapter 20 - Embryology of The Genitourinary Tract - Campbell - Walsh-Wein UROLOGY 12thDocumento40 pagineChapter 20 - Embryology of The Genitourinary Tract - Campbell - Walsh-Wein UROLOGY 12thkrisnaNessuna valutazione finora
- Format Ketikan LabDocumento9 pagineFormat Ketikan Labapril babyNessuna valutazione finora
- Parenting Children With Reactive Attachment DisorderDocumento13 pagineParenting Children With Reactive Attachment Disorderboglous100% (1)
- Xi - Bio Zoo Question PaperDocumento9 pagineXi - Bio Zoo Question PaperVeeramaniNessuna valutazione finora
- ReceptoretDocumento37 pagineReceptoretBlodin ZylfiuNessuna valutazione finora
- Problem Set 2 EndocrinologyDocumento12 pagineProblem Set 2 EndocrinologyJessica EtieneNessuna valutazione finora
- Neonatal JaundiceDocumento56 pagineNeonatal Jaundicesuardiman acoNessuna valutazione finora
- Melatonin Disturbances in Anorexia Nervosa and Bulimia NervosaDocumento9 pagineMelatonin Disturbances in Anorexia Nervosa and Bulimia NervosaImelia AnggraeniNessuna valutazione finora
- Fluids and Transport: Fundamentals of Anatomy & PhysiologyDocumento161 pagineFluids and Transport: Fundamentals of Anatomy & Physiologyann aquinoNessuna valutazione finora
- Bloody Tears Following Lefort 1Documento3 pagineBloody Tears Following Lefort 1paulwhite1234Nessuna valutazione finora
- Chapter 18 - Apoptosis - 112612Documento28 pagineChapter 18 - Apoptosis - 112612Anonymous nkR1PhIHNessuna valutazione finora
- Li 1 Anatomy, Histology, PhysiologyDocumento17 pagineLi 1 Anatomy, Histology, PhysiologysandyaadindaNessuna valutazione finora
- Type of Cell FunctionDocumento3 pagineType of Cell FunctionDerek Pagsolingan0% (1)
- Emma Jordan - Research Final DraftDocumento7 pagineEmma Jordan - Research Final Draftapi-436829682Nessuna valutazione finora
- Australian Prescriber (1988) Bioavailability and First Past ClearanceDocumento3 pagineAustralian Prescriber (1988) Bioavailability and First Past Clearance1234chocoNessuna valutazione finora
- ADR Common Drug - Induced Organ DisordersDocumento45 pagineADR Common Drug - Induced Organ Disorders0009439Nessuna valutazione finora