Potrebbero piacerti anche
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Pilar Cyst With CrystalsDocumento2 paginePilar Cyst With CrystalsDeba P SarmaNessuna valutazione finora
- Acantholytic Solar Keratosis, M 67, Forehead PDFDocumento6 pagineAcantholytic Solar Keratosis, M 67, Forehead PDFDeba P SarmaNessuna valutazione finora
- Acantholytic Dermatosis With DyskeratosisDocumento11 pagineAcantholytic Dermatosis With DyskeratosisDeba P SarmaNessuna valutazione finora
- Accessory TragusDocumento3 pagineAccessory TragusDeba P SarmaNessuna valutazione finora
- Acantholytic Bullous DiseaseDocumento4 pagineAcantholytic Bullous DiseaseDeba P SarmaNessuna valutazione finora
- Acantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Documento3 pagineAcantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Deba P SarmaNessuna valutazione finora
- Acantholytic Actinic KeratosisDocumento4 pagineAcantholytic Actinic KeratosisDeba P SarmaNessuna valutazione finora
- Xanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDocumento7 pagineXanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDeba P SarmaNessuna valutazione finora
- Balanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Documento6 pagineBalanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Deba P SarmaNessuna valutazione finora
- Results of Search in Google Scholar On 'Deba P Sarma'Documento28 pagineResults of Search in Google Scholar On 'Deba P Sarma'Deba P SarmaNessuna valutazione finora
- Verrucous Carcinoma of The Foot, M 63, Left FootDocumento8 pagineVerrucous Carcinoma of The Foot, M 63, Left FootDeba P Sarma100% (1)
- Acantholytic Acanthoma. M 60, ScrotumDocumento8 pagineAcantholytic Acanthoma. M 60, ScrotumDeba P SarmaNessuna valutazione finora
- Xanthogranuloma, M 30, Right ElbowDocumento4 pagineXanthogranuloma, M 30, Right ElbowDeba P SarmaNessuna valutazione finora
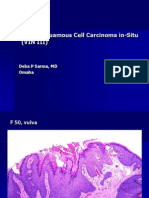
- Vulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDocumento6 pagineVulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDeba P SarmaNessuna valutazione finora
- Xanthogranuloma PPT DSDocumento9 pagineXanthogranuloma PPT DSDeba P SarmaNessuna valutazione finora
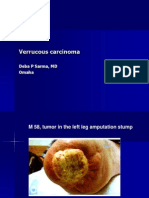
- Verrucous Carcinoma., M 58, Left Leg Amputation StumpDocumento7 pagineVerrucous Carcinoma., M 58, Left Leg Amputation StumpDeba P SarmaNessuna valutazione finora
- Verrucous Epidermal Nevus. F 43, ScalpDocumento4 pagineVerrucous Epidermal Nevus. F 43, ScalpDeba P SarmaNessuna valutazione finora
- Verruca Vulgaris., M 22.,PPTDocumento2 pagineVerruca Vulgaris., M 22.,PPTDeba P SarmaNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Inverse Curve Trip Time Calculation: Enter Values in White CellDocumento3 pagineInverse Curve Trip Time Calculation: Enter Values in White CellVijay FxNessuna valutazione finora
- WPCE Wireline Lubricator With Threaded Unions PDFDocumento1 paginaWPCE Wireline Lubricator With Threaded Unions PDFDidik safdaliNessuna valutazione finora
- Application of Eye Patch, Eye Shield and Pressure Dressing To The EyeDocumento2 pagineApplication of Eye Patch, Eye Shield and Pressure Dressing To The EyeissaiahnicolleNessuna valutazione finora
- BRASS Introduction 2012Documento23 pagineBRASS Introduction 20121234scr5678Nessuna valutazione finora
- NDT Matrix 12-99-90-1710 - Rev.2 PDFDocumento2 pagineNDT Matrix 12-99-90-1710 - Rev.2 PDFEPC NCCNessuna valutazione finora
- 3TRIGODocumento5 pagine3TRIGOCielo Pabilan ObemioNessuna valutazione finora
- Original Sandeha NivariniDocumento117 pagineOriginal Sandeha NivariniHmis BlrNessuna valutazione finora
- Water Sensitive Urban Design GuidelineDocumento42 pagineWater Sensitive Urban Design GuidelineTri Wahyuningsih100% (1)
- Advanced Aesthetics: The Definitive Guide For Building A Ripped and Muscular PhysiqueDocumento73 pagineAdvanced Aesthetics: The Definitive Guide For Building A Ripped and Muscular PhysiqueRoger murilloNessuna valutazione finora
- JMO 2023 (7, 8) Question PaperDocumento2 pagineJMO 2023 (7, 8) Question PaperSuryanshu BhardwajNessuna valutazione finora
- Spina 2002Documento10 pagineSpina 2002hasantapNessuna valutazione finora
- The Hollow Boy Excerpt PDFDocumento52 pagineThe Hollow Boy Excerpt PDFCathy Mars100% (1)
- Bahasa Inggris PATDocumento10 pagineBahasa Inggris PATNilla SumbuasihNessuna valutazione finora
- Nitrogen CycleDocumento12 pagineNitrogen Cycleasa bspcpkNessuna valutazione finora
- Chemistry Jun 2010 Mark Scheme Unit 3Documento15 pagineChemistry Jun 2010 Mark Scheme Unit 3dylandonNessuna valutazione finora
- مستر رمضان عوضDocumento24 pagineمستر رمضان عوضSamuel SaadNessuna valutazione finora
- 5 160 1 PBDocumento13 pagine5 160 1 PBLotkomoaidone Harahu TukambaNessuna valutazione finora
- Fo Transfer ProcedureDocumento8 pagineFo Transfer ProcedureadityasahayNessuna valutazione finora
- Neuropsychological Performance in Neurofibromatosis Type 1: Original ArticleDocumento5 pagineNeuropsychological Performance in Neurofibromatosis Type 1: Original ArticleRaquel DuarteNessuna valutazione finora
- The Common Reader-Virginia WoolfDocumento216 pagineThe Common Reader-Virginia WoolfRusudan VardiashviliNessuna valutazione finora
- Cho Gsas - Harvard 0084L 11462Documento503 pagineCho Gsas - Harvard 0084L 11462Claudemiro costaNessuna valutazione finora
- Manual de Electronica HardbookDocumento970 pagineManual de Electronica HardbookninoferNessuna valutazione finora
- Mathematics 7 LAS Quarter 3Documento97 pagineMathematics 7 LAS Quarter 3Villamor Baculi82% (17)
- Hyundai Forklift Catalog PTASDocumento15 pagineHyundai Forklift Catalog PTASjack comboNessuna valutazione finora
- Need For Advanced Suspension SystemsDocumento10 pagineNeed For Advanced Suspension SystemsIQPC GmbHNessuna valutazione finora
- Greek ArchitectureDocumento16 pagineGreek ArchitectureXlyth RodriguezNessuna valutazione finora
- Famous Bombers of The Second World War - 1st SeriesDocumento142 pagineFamous Bombers of The Second World War - 1st Seriesgunfighter29100% (1)
- CSEC Chemistry June 2018 P2 AnswersDocumento7 pagineCSEC Chemistry June 2018 P2 AnswerscxcchemistryNessuna valutazione finora
- Module 02 Connect Hardware Peripherals EndaleDocumento49 pagineModule 02 Connect Hardware Peripherals EndaleSoli Mondo100% (1)