Potrebbero piacerti anche
- 9 April 2019Documento1 pagina9 April 2019Cherry Oña AntoninoNessuna valutazione finora
- Che RLDocumento2 pagineChe RLCherry Oña AntoninoNessuna valutazione finora
- Visiting TimeDocumento1 paginaVisiting TimeCherry Oña AntoninoNessuna valutazione finora
- 16 March 2021Documento1 pagina16 March 2021Cherry Oña AntoninoNessuna valutazione finora
- Maternity LeaveDocumento1 paginaMaternity LeaveCherry Oña AntoninoNessuna valutazione finora
- 9 April 2019Documento1 pagina9 April 2019Cherry Oña AntoninoNessuna valutazione finora
- Che RLDocumento2 pagineChe RLCherry Oña AntoninoNessuna valutazione finora
- Critical Care Calculations Study GuideDocumento6 pagineCritical Care Calculations Study GuideAja Blue100% (2)
- Che RLDocumento2 pagineChe RLCherry Oña AntoninoNessuna valutazione finora
- Letter PNCDocumento1 paginaLetter PNCCherry Oña AntoninoNessuna valutazione finora
- Grgert 5Documento47 pagineGrgert 5Cherry Oña AntoninoNessuna valutazione finora
- Feeding Guidelines For Infants: 500-599Documento1 paginaFeeding Guidelines For Infants: 500-599Cherry Oña AntoninoNessuna valutazione finora
- Grgert 5Documento47 pagineGrgert 5Cherry Oña AntoninoNessuna valutazione finora
- JKGGGDocumento2 pagineJKGGGCherry Oña AntoninoNessuna valutazione finora
- Operating Room Procedureguidelines: Arthroscopy (Shoulder, Elbow, Wrist, Hip, & Knee)Documento11 pagineOperating Room Procedureguidelines: Arthroscopy (Shoulder, Elbow, Wrist, Hip, & Knee)Cherry Oña AntoninoNessuna valutazione finora
- Second Edition Prometric 2013-More Than 500 QDocumento131 pagineSecond Edition Prometric 2013-More Than 500 QNeelamBadruddin77% (13)
- Second Edition Prometric 2013-More Than 500 QDocumento131 pagineSecond Edition Prometric 2013-More Than 500 QNeelamBadruddin77% (13)
- Letter PNCDocumento1 paginaLetter PNCCherry Oña AntoninoNessuna valutazione finora
- JKGGGDocumento2 pagineJKGGGCherry Oña AntoninoNessuna valutazione finora
- SCFHS Faq PDFDocumento3 pagineSCFHS Faq PDFJiby MathewNessuna valutazione finora
- Che RLDocumento2 pagineChe RLCherry Oña AntoninoNessuna valutazione finora
- 19 December 2018Documento1 pagina19 December 2018Cherry Oña AntoninoNessuna valutazione finora
- Guidelines For NursesDocumento1 paginaGuidelines For NursesCherry Oña AntoninoNessuna valutazione finora
- Che RLDocumento2 pagineChe RLCherry Oña AntoninoNessuna valutazione finora
- DTR SingleDocumento2 pagineDTR SingleCherry Oña AntoninoNessuna valutazione finora
- Guidelines For NursesDocumento18 pagineGuidelines For NursesBASKORO AbdiansyahNessuna valutazione finora
- SopranoDocumento1 paginaSopranoCherry Oña AntoninoNessuna valutazione finora
- Evaluation Sheet For Final DemoDocumento3 pagineEvaluation Sheet For Final DemoCherry Oña AntoninoNessuna valutazione finora
- Detailed Lesson Plan EspDocumento3 pagineDetailed Lesson Plan EspCherry Oña Antonino100% (5)
- Meaning of Office FurnitureDocumento2 pagineMeaning of Office FurnitureCherry Oña AntoninoNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Monitor Zoncare - PM-8000 ServicemanualDocumento83 pagineMonitor Zoncare - PM-8000 Servicemanualwilmer100% (1)
- 756S PDFDocumento248 pagine756S PDFShahzad FidaNessuna valutazione finora
- Case Analysis of Vishal Jeet V. Union of India Trafficking of Women and ChildrenDocumento7 pagineCase Analysis of Vishal Jeet V. Union of India Trafficking of Women and ChildrenTrishani NahaNessuna valutazione finora
- Gulayan Sa Barangay OrdinanceDocumento2 pagineGulayan Sa Barangay OrdinancekonsinoyeNessuna valutazione finora
- Barangay Clearance SampleDocumento1 paginaBarangay Clearance SampleBarangay Onse Malaybalay100% (3)
- Governance, Business Ethics, Risk Management and Internal ControlDocumento4 pagineGovernance, Business Ethics, Risk Management and Internal ControlJosua PagcaliwaganNessuna valutazione finora
- Diabetes Mellitus Nursing Care PlanDocumento7 pagineDiabetes Mellitus Nursing Care PlanjamieboyRN91% (32)
- Web Script Ems Core 4 Hernandez - Gene Roy - 07!22!2020Documento30 pagineWeb Script Ems Core 4 Hernandez - Gene Roy - 07!22!2020gene roy hernandezNessuna valutazione finora
- Surgical Management in LeprosyDocumento33 pagineSurgical Management in Leprosynsv.epicNessuna valutazione finora
- Adhi Wardana 405120042: Blok PenginderaanDocumento51 pagineAdhi Wardana 405120042: Blok PenginderaanErwin DiprajaNessuna valutazione finora
- Io (Jupiter Moon)Documento2 pagineIo (Jupiter Moon)FatimaNessuna valutazione finora
- Implementing Self-Administration of Insulin in Hospital: A Journey of Discovery and Innovation. Part 1: Culture and StorageDocumento4 pagineImplementing Self-Administration of Insulin in Hospital: A Journey of Discovery and Innovation. Part 1: Culture and Storagesunrise755Nessuna valutazione finora
- Profile of RespondentsDocumento36 pagineProfile of RespondentsPratibha SharmaNessuna valutazione finora
- Writing The Motherland From The DiasporaDocumento23 pagineWriting The Motherland From The DiasporaIfeoluwa Watson100% (1)
- Labor Case DigestDocumento2 pagineLabor Case DigestJhollinaNessuna valutazione finora
- Molecular MechanicsDocumento26 pagineMolecular MechanicsKarthi ShanmugamNessuna valutazione finora
- The Nursing ShortageDocumento6 pagineThe Nursing Shortageapi-455495817Nessuna valutazione finora
- A Walk in The Physical - Christian SundbergDocumento282 pagineA Walk in The Physical - Christian SundbergKatie MhNessuna valutazione finora
- Kerala Medico Legal Code - Annexure2Documento19 pagineKerala Medico Legal Code - Annexure2doctor82Nessuna valutazione finora
- Muet Topic 10 City Life Suggested Answer and IdiomsDocumento3 pagineMuet Topic 10 City Life Suggested Answer and IdiomsMUHAMAD FAHMI BIN SHAMSUDDIN MoeNessuna valutazione finora
- A Guide To LU3 PDFDocumento54 pagineA Guide To LU3 PDFMigs MedinaNessuna valutazione finora
- - 50 Đề Thi Học Sinh Gioi Lớp 12Documento217 pagine- 50 Đề Thi Học Sinh Gioi Lớp 12Nguyễn Thanh ThảoNessuna valutazione finora
- Chapter 23Documento9 pagineChapter 23Trixie Myr AndoyNessuna valutazione finora
- Contoh Perhitungan DDD Excell - IRNADocumento8 pagineContoh Perhitungan DDD Excell - IRNAMaya DamanikNessuna valutazione finora
- 08 163 4 JPL ScheickDocumento50 pagine08 163 4 JPL ScheickSaqib Ali KhanNessuna valutazione finora
- VSR 411 QB AnaesthesiaDocumento7 pagineVSR 411 QB Anaesthesiavishnu dathNessuna valutazione finora
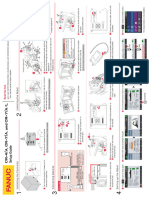
- CR-7iA CR-4iA Installation and Setup Guide (B-83774JA-1 01)Documento1 paginaCR-7iA CR-4iA Installation and Setup Guide (B-83774JA-1 01)lidiia.pavlkukNessuna valutazione finora
- Hedayati2014 Article BirdStrikeAnalysisOnATypicalHeDocumento12 pagineHedayati2014 Article BirdStrikeAnalysisOnATypicalHeSharan KharthikNessuna valutazione finora
- February 2023 PROGRAM OF THE MPLEDocumento8 pagineFebruary 2023 PROGRAM OF THE MPLEDale Iverson LacastreNessuna valutazione finora
- RA ELECTRONICSTECH CEBU Apr2019 PDFDocumento12 pagineRA ELECTRONICSTECH CEBU Apr2019 PDFPhilBoardResultsNessuna valutazione finora