Potrebbero piacerti anche
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Vectorial Analysis of Ecg: Learning ObjectivesDocumento8 pagineVectorial Analysis of Ecg: Learning ObjectivesMukesh GuptaNessuna valutazione finora
- Bioenergetics DLLDocumento2 pagineBioenergetics DLLAlvin PaboresNessuna valutazione finora
- Inotozumab OzogamicinDocumento14 pagineInotozumab OzogamicinTaraNessuna valutazione finora
- PH SalivaDocumento5 paginePH SalivaBia KneippNessuna valutazione finora
- 11th International Symposium On Urolithiasis Nice France 25 Sept 2008Documento76 pagine11th International Symposium On Urolithiasis Nice France 25 Sept 2008assemNessuna valutazione finora
- Achy Breaky HeartDocumento2 pagineAchy Breaky Heartapi-3810640Nessuna valutazione finora
- Senior Biology 1 Q1 - M9 For PrintingDocumento41 pagineSenior Biology 1 Q1 - M9 For PrintingMARIBETH RAMOSNessuna valutazione finora
- Local Media5318352258259372198Documento23 pagineLocal Media5318352258259372198Marie LlanesNessuna valutazione finora
- BAI TAP ON VE DAU TRONG AM - TU CO 3 AM TIET (CO DAP AN) - T I 123doc - VNDocumento3 pagineBAI TAP ON VE DAU TRONG AM - TU CO 3 AM TIET (CO DAP AN) - T I 123doc - VNNgô Huyền ThươngNessuna valutazione finora
- Cloning: Kabindra SahuDocumento37 pagineCloning: Kabindra SahuKabindra SahooNessuna valutazione finora
- Animals With 5 Legs - Google SearchDocumento1 paginaAnimals With 5 Legs - Google SearchBen BerardNessuna valutazione finora
- PHOTOSYNTESISDocumento23 paginePHOTOSYNTESISJustine Kate PurisimaNessuna valutazione finora
- Biology Chapter 2 Sexual Reproduction in Flowering PlantsDocumento8 pagineBiology Chapter 2 Sexual Reproduction in Flowering PlantsYasir SalahNessuna valutazione finora
- Lecture 3 Genetic CounselingDocumento23 pagineLecture 3 Genetic Counselingimorkzone100% (1)
- Cats Are Not PeaDocumento294 pagineCats Are Not PeaMirabella AstraNessuna valutazione finora
- Cephalometric Analysis Manual Tracing of A LateralDocumento5 pagineCephalometric Analysis Manual Tracing of A Lateralmoh.ahm3040Nessuna valutazione finora
- Workup For ProteinuriaDocumento17 pagineWorkup For ProteinuriaSantiago ChávezNessuna valutazione finora
- Yoga Massage Therapy BookDocumento54 pagineYoga Massage Therapy BookKhadi MadamaNessuna valutazione finora
- % Chapter 2 Regulation of Body Temperature: Multiple-Choice QuestionsDocumento32 pagine% Chapter 2 Regulation of Body Temperature: Multiple-Choice QuestionsK C100% (1)
- Nutrition in Plants - Mineral Nutrition: Module - 2Documento13 pagineNutrition in Plants - Mineral Nutrition: Module - 2keerthyNessuna valutazione finora
- Global Forest Resources Assessment - Sri LankaDocumento55 pagineGlobal Forest Resources Assessment - Sri LankaTilak ConradNessuna valutazione finora
- Principles of Keyline DesignDocumento2 paginePrinciples of Keyline Designinfo1381Nessuna valutazione finora
- Hl7 Human r3Documento1 paginaHl7 Human r3orsis teknıkNessuna valutazione finora
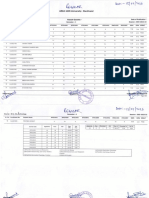
- Result Gazette Regular ODD 22 23 1st Semester B.SC Biotechnology. 1Documento2 pagineResult Gazette Regular ODD 22 23 1st Semester B.SC Biotechnology. 1Abhishek BhaduriNessuna valutazione finora
- Banana - WikipediaDocumento33 pagineBanana - WikipediaBryan Paul BautistaNessuna valutazione finora
- Pengembangan Sediaan Vitamin C Lepas Lambat Dengan Pemanfaatan Material Nanosilika DAUN BAMBU (Bambusa SP.)Documento10 paginePengembangan Sediaan Vitamin C Lepas Lambat Dengan Pemanfaatan Material Nanosilika DAUN BAMBU (Bambusa SP.)hanifahNessuna valutazione finora
- MD Simulation Tutorial in GromacsDocumento9 pagineMD Simulation Tutorial in GromacsSimanta PaulNessuna valutazione finora
- Observations - Project Chadín 2 - Flora y Fauna PDFDocumento36 pagineObservations - Project Chadín 2 - Flora y Fauna PDFGuido Erlin Araujo0% (1)
- Formulation and Evaluation of Floating in Situ Gel Based Gastroretentive Drug Delivery of Ciprofloxacin HCLDocumento11 pagineFormulation and Evaluation of Floating in Situ Gel Based Gastroretentive Drug Delivery of Ciprofloxacin HCLiajpsNessuna valutazione finora
- 1 s2.0 S0925521404002017 Main PDFDocumento7 pagine1 s2.0 S0925521404002017 Main PDFJefferson Bittencourt VenâncioNessuna valutazione finora