Potrebbero piacerti anche
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Secondary Amenorrhea Testing AlgorithmDocumento1 paginaSecondary Amenorrhea Testing AlgorithmpolygoneNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Recent Advancement in Infertility ManagementDocumento18 pagineRecent Advancement in Infertility ManagementFarheen khan100% (2)
- Fertility and SubfertilityDocumento95 pagineFertility and SubfertilitydidiNessuna valutazione finora
- LESSON PLAN For COTDocumento5 pagineLESSON PLAN For COTMerrie Anne Pascual BagsicNessuna valutazione finora
- InfertilityDocumento10 pagineInfertilityits_piks7256Nessuna valutazione finora
- A Study To Assess The Effectiveness of Structured Teaching Programme On Pregnancy Induced Hypertension Among Antenatal Mothers in Selected Areas of RaichurDocumento19 pagineA Study To Assess The Effectiveness of Structured Teaching Programme On Pregnancy Induced Hypertension Among Antenatal Mothers in Selected Areas of Raichursanvar soniNessuna valutazione finora
- Chlamydia SlidesDocumento63 pagineChlamydia Slideslia primasari100% (1)
- Responsible Parenthood and Reproductive Health:: Family PlanningDocumento37 pagineResponsible Parenthood and Reproductive Health:: Family PlanningalyssaNessuna valutazione finora
- M Vanguardia-McnpDocumento11 pagineM Vanguardia-Mcnpmark OrpillaNessuna valutazione finora
- Management of Bleeding in Early PregnancyDocumento44 pagineManagement of Bleeding in Early PregnancyOyedele OluwaseunNessuna valutazione finora
- Department of Education: Learning Activity Sheet in Science 6Documento4 pagineDepartment of Education: Learning Activity Sheet in Science 6Tampok ES (Region III - Bulacan)Nessuna valutazione finora
- Pretest and PosttestDocumento3 paginePretest and PosttestMarissa FontanilNessuna valutazione finora
- New Estrogen and ProgesteroneDocumento39 pagineNew Estrogen and ProgesteroneWegrimel AriegaraNessuna valutazione finora
- 75 - PDFsam - GOMELLA 14Documento18 pagine75 - PDFsam - GOMELLA 14Chago MencosNessuna valutazione finora
- The Breasts Do Become Sensitive and Some Women DoDocumento14 pagineThe Breasts Do Become Sensitive and Some Women DoJaymih Santos AbasoloNessuna valutazione finora
- DR Case Pres Updated 1Documento30 pagineDR Case Pres Updated 1Ethan NamoNessuna valutazione finora
- Maternal and Child Nursing - Antenatal Practice Test With Answers and RationaleDocumento31 pagineMaternal and Child Nursing - Antenatal Practice Test With Answers and Rationalegelean payodNessuna valutazione finora
- Anatomy and Physiology: Patient P / Room No. 415 - 1Documento3 pagineAnatomy and Physiology: Patient P / Room No. 415 - 1Julianne B. Dela Cruz100% (1)
- Telaah JurnalDocumento5 pagineTelaah JurnalMade Angga DiningratNessuna valutazione finora
- RMS Senior B WangayaDocumento11 pagineRMS Senior B Wangayaimamsantos1191Nessuna valutazione finora
- guigoz milk - ស្វែងរក GoogleDocumento1 paginaguigoz milk - ស្វែងរក Googlelammei6868Nessuna valutazione finora
- Molar PregnancyDocumento15 pagineMolar Pregnancyapi-3705046Nessuna valutazione finora
- Newborn AssessmentDocumento3 pagineNewborn AssessmentMimie CaliNessuna valutazione finora
- Subamniotic Hematoma: Case Report and Review of LiteratureDocumento3 pagineSubamniotic Hematoma: Case Report and Review of LiteratureIJAR JOURNALNessuna valutazione finora
- Research Proposal o NishaDocumento14 pagineResearch Proposal o NishaNishaThakuri100% (1)
- Week 3 - MenstruationDocumento10 pagineWeek 3 - MenstruationTEDDY BEAR PRODUCTIONNessuna valutazione finora
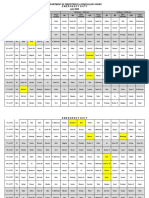
- Department of Obstetrics & Gynecology-Wwrc Emergency Duty July 2020Documento3 pagineDepartment of Obstetrics & Gynecology-Wwrc Emergency Duty July 2020noorNessuna valutazione finora
- Evaluation of The Endometrium For Malignant or Premalignant DiseaseDocumento10 pagineEvaluation of The Endometrium For Malignant or Premalignant Diseasenautilus81Nessuna valutazione finora
- Obstetric Haemorrhage: EsmoeDocumento40 pagineObstetric Haemorrhage: EsmoePoonam RanaNessuna valutazione finora
- In-Vitro Fertilisation (Ivf) in Singapore: Charges and Success RatesDocumento4 pagineIn-Vitro Fertilisation (Ivf) in Singapore: Charges and Success RatesLászló ÉvaNessuna valutazione finora