Potrebbero piacerti anche
- Insight, Empathy and Alienation in Heidegger's Being and TimeDocumento23 pagineInsight, Empathy and Alienation in Heidegger's Being and TimeIan Rory OwenNessuna valutazione finora
- Heidegger On EmpathyDocumento21 pagineHeidegger On EmpathyIan Rory OwenNessuna valutazione finora
- On Existential TherapyDocumento22 pagineOn Existential TherapyIan Rory Owen100% (1)
- Husserl On EmpathyDocumento22 pagineHusserl On EmpathyIan Rory Owen100% (1)
- IntersubjectivityDocumento8 pagineIntersubjectivityIan Rory Owen100% (1)
- Edmund Husserl's PhenomenologyDocumento11 pagineEdmund Husserl's PhenomenologyIan Rory Owen100% (3)
- 6th Central Pay Commission Salary CalculatorDocumento15 pagine6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Assignment Day 1 UHV - V4Documento3 pagineAssignment Day 1 UHV - V4adaily life100% (1)
- DEATH StudeDocumento32 pagineDEATH StudeGlenn AltarNessuna valutazione finora
- Marie Yvette C. Alcazar UP College of EducationDocumento11 pagineMarie Yvette C. Alcazar UP College of EducationMa Crimeldy Portunova-GaporNessuna valutazione finora
- Definition of Terms in Practical Research 1Documento2 pagineDefinition of Terms in Practical Research 1Alyssa JaneNessuna valutazione finora
- NSTP 1 Prelim Quiz 2 To Prelim ExamDocumento21 pagineNSTP 1 Prelim Quiz 2 To Prelim ExamJOSHUA PALMANessuna valutazione finora
- Third Grade Social Studies Lesson PlanDocumento3 pagineThird Grade Social Studies Lesson Planapi-600745006Nessuna valutazione finora
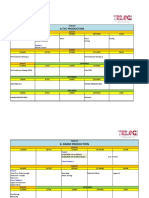
- Timeline Production TVC, Radio & Jingle PDFDocumento3 pagineTimeline Production TVC, Radio & Jingle PDFMichael FerdyNessuna valutazione finora
- The World of Apu - RayDocumento21 pagineThe World of Apu - Rayjim kistenNessuna valutazione finora
- Social Skills SundeepDocumento10 pagineSocial Skills SundeepKomal KhatterNessuna valutazione finora
- Final Essay - Discuss The Relationship Between Intelligence and Creativity 2 PDFDocumento7 pagineFinal Essay - Discuss The Relationship Between Intelligence and Creativity 2 PDFGRACE ON SPILLNessuna valutazione finora
- 1st Quarterly Examination in DIASSDocumento4 pagine1st Quarterly Examination in DIASSAngelo LlanosNessuna valutazione finora
- What Is CounselingDocumento2 pagineWhat Is CounselingJethro Earl VergaraNessuna valutazione finora
- Bullying-Series-Part-2 - 2Documento2 pagineBullying-Series-Part-2 - 2Tatuka Gogolidze100% (1)
- Le Cirque Des RêvesDocumento12 pagineLe Cirque Des RêvesGabriel VillagomezNessuna valutazione finora
- L11 - The Five SkhandasDocumento12 pagineL11 - The Five SkhandasAditya MudNessuna valutazione finora
- Post Box Lesson PlanDocumento1 paginaPost Box Lesson PlanLouise Robinson-LayNessuna valutazione finora
- Baby Enur N. Jao Philosophy Abm 12 B Engaging ActivityDocumento2 pagineBaby Enur N. Jao Philosophy Abm 12 B Engaging ActivityJAO BABY ENURNessuna valutazione finora
- Health Module 6 g7Documento26 pagineHealth Module 6 g7Richelle PamintuanNessuna valutazione finora
- Directing Actors ChartDocumento1 paginaDirecting Actors ChartNag Vardhan100% (1)
- Individual Work On Team RubricDocumento1 paginaIndividual Work On Team RubricJimmary MonongNessuna valutazione finora
- FS2 EP3 (Gregori, BEED 4-A)Documento14 pagineFS2 EP3 (Gregori, BEED 4-A)Sheina Gregori100% (2)
- PPT - Ch06 - Proses Kaunseling Dan PenamatanDocumento40 paginePPT - Ch06 - Proses Kaunseling Dan PenamatanSreednesh A/l MurthyNessuna valutazione finora
- DLL - Mathematics 5 - Q4 - W4Documento7 pagineDLL - Mathematics 5 - Q4 - W4Gisselle BadanaNessuna valutazione finora
- Evaluation Techniques: Human-Computer InteractionDocumento22 pagineEvaluation Techniques: Human-Computer InteractionKristine Karylle NeveridaNessuna valutazione finora
- Understanding The Self - Unit 1 DoneDocumento33 pagineUnderstanding The Self - Unit 1 DoneKyll HernandezNessuna valutazione finora
- Learning Activity Exercise NoDocumento8 pagineLearning Activity Exercise NoCindy MariscotesNessuna valutazione finora
- Student Centered and or Differentiated Instruction - Reflection and RationaleDocumento5 pagineStudent Centered and or Differentiated Instruction - Reflection and Rationaleapi-486184360Nessuna valutazione finora
- Students' Coping Mechanisms On The Academic StressDocumento10 pagineStudents' Coping Mechanisms On The Academic Stresstoariel.delacruzjrNessuna valutazione finora
- Rics RRLDocumento7 pagineRics RRLDianne Mei Tagabi CastroNessuna valutazione finora
- An Exploration of Self Fulfillment in Vikram Seth's Select Novels The Golden Gate and A Suitable BoyDocumento4 pagineAn Exploration of Self Fulfillment in Vikram Seth's Select Novels The Golden Gate and A Suitable BoyEditor IJTSRDNessuna valutazione finora