Potrebbero piacerti anche
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsNessuna valutazione finora
- Cardiac Tamponade, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandCardiac Tamponade, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Sick Sinus Syndrome, (Sinus Nodal Disorder) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandSick Sinus Syndrome, (Sinus Nodal Disorder) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- A Simple Guide to Pneumothorax (Collapsed Lungs), Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Pneumothorax (Collapsed Lungs), Diagnosis, Treatment and Related ConditionsNessuna valutazione finora
- Chest Tube Drainage of The Pleural SpaceDocumento10 pagineChest Tube Drainage of The Pleural SpaceFernandaNessuna valutazione finora
- Anemia in CKD Patient On HeamodialysisDocumento32 pagineAnemia in CKD Patient On HeamodialysisEditor IJTSRDNessuna valutazione finora
- ECG Study GuideDocumento7 pagineECG Study GuideannaNessuna valutazione finora
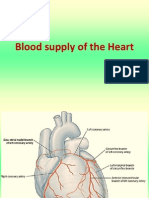
- Blood Supply of HeartDocumento7 pagineBlood Supply of Heartmariposa_0612Nessuna valutazione finora
- Management of Hypertension: Affan Syafiqi - Nurul Husna - Audi RahmanDocumento77 pagineManagement of Hypertension: Affan Syafiqi - Nurul Husna - Audi RahmanRavi K. ShuklaNessuna valutazione finora
- Pediatric Shock: A Guide to Identification, Classification and Initial ManagementDocumento20 paginePediatric Shock: A Guide to Identification, Classification and Initial ManagementvgmanjunathNessuna valutazione finora
- EdemaDocumento3 pagineEdemaUdaya SreeNessuna valutazione finora
- Transposition of The Great VesselDocumento30 pagineTransposition of The Great VesseljustinahorroNessuna valutazione finora
- Acidosis and AlkolosisDocumento4 pagineAcidosis and AlkolosisDani PhilipNessuna valutazione finora
- Anterior Cord SyndromeDocumento8 pagineAnterior Cord SyndromeJanine Erika Julom BrillantesNessuna valutazione finora
- Cor Pulmonale: Dr. Gerrard UyDocumento13 pagineCor Pulmonale: Dr. Gerrard Uyfaridah azzah sariNessuna valutazione finora
- Cardiac Examination Inspection, Palpation & Percussion : Dr. Rajesh Bhat UDocumento38 pagineCardiac Examination Inspection, Palpation & Percussion : Dr. Rajesh Bhat URanjith RavellaNessuna valutazione finora
- Understanding Subdural Hematomas - Causes, Symptoms and TreatmentDocumento54 pagineUnderstanding Subdural Hematomas - Causes, Symptoms and TreatmentNuzhat Noor Ayesha100% (1)
- Surgical Treatment For BREAST CANCERDocumento5 pagineSurgical Treatment For BREAST CANCERJericho James TopacioNessuna valutazione finora
- Predisposing Conditions, Management and Prevention of Chronic Kidney DiseaseDocumento52 paginePredisposing Conditions, Management and Prevention of Chronic Kidney DiseaseSaad MotawéaNessuna valutazione finora
- Etiology and Diagnosis of Bile Duct StonesDocumento8 pagineEtiology and Diagnosis of Bile Duct Stoneskuncupcupu1368Nessuna valutazione finora
- Ascitic Fluid AnalysisDocumento3 pagineAscitic Fluid AnalysisLohJNessuna valutazione finora
- Shock Power PointDocumento24 pagineShock Power PointmarwaNessuna valutazione finora
- Coronary Artery Disease Cad2Documento182 pagineCoronary Artery Disease Cad2Mamot MotNessuna valutazione finora
- Pediatric Vital Signs MeasurementsDocumento3 paginePediatric Vital Signs MeasurementsJheDelaPazValenzuelaNessuna valutazione finora
- Clinical Management: PGI Eileen Andres PediatricsDocumento9 pagineClinical Management: PGI Eileen Andres PediatricsMichael BonillaNessuna valutazione finora
- Myocardial InfarctionDocumento18 pagineMyocardial InfarctionYanna Habib-MangotaraNessuna valutazione finora
- Abdominal Trauma Signs, Symptoms and Nursing CareDocumento24 pagineAbdominal Trauma Signs, Symptoms and Nursing CareSurgeryClassesNessuna valutazione finora
- Epidural Hematoma: Kurniasari Armayana AhmadDocumento10 pagineEpidural Hematoma: Kurniasari Armayana AhmadSuci AlimaNessuna valutazione finora
- MINI CP Angina PectorisDocumento11 pagineMINI CP Angina Pectorisyasira100% (1)
- ICU Case Study: 53-Year-Old Male with Organophosphate PoisoningDocumento11 pagineICU Case Study: 53-Year-Old Male with Organophosphate PoisoningPrasyaanth RajanNessuna valutazione finora
- PARAQUAT POISIONING 3rd Block Imed COMPLIEDDocumento15 paginePARAQUAT POISIONING 3rd Block Imed COMPLIEDMohil PratapNessuna valutazione finora
- Pathophysiology of Atrial FibrillationDocumento12 paginePathophysiology of Atrial FibrillationAndrew Surya Putra SccNessuna valutazione finora
- Diagnostic Test For Heart DiseasesDocumento16 pagineDiagnostic Test For Heart DiseasesJaimee Jonah ChristieNessuna valutazione finora
- Pulmonary Rehabilitation PPDocumento19 paginePulmonary Rehabilitation PPnashqonashNessuna valutazione finora
- Congenital Heart DiseasesDocumento21 pagineCongenital Heart DiseasesfahmiNessuna valutazione finora
- Arterial Blood Gases: A Step by Step GuideDocumento19 pagineArterial Blood Gases: A Step by Step GuideKathleen Ann50% (2)
- Chapter 2Documento14 pagineChapter 2api-294209774100% (1)
- Coarctation of The AortaDocumento7 pagineCoarctation of The Aortamharz_astillo100% (1)
- Ulcerative Colitis: DR Syed Ubaid Associate Professor of SurgeryDocumento71 pagineUlcerative Colitis: DR Syed Ubaid Associate Professor of SurgeryFachry Al RafiqiNessuna valutazione finora
- Subdural Hematomas in the Elderly: Diagnosis and Treatment of the Great Neurological ImitatorDocumento19 pagineSubdural Hematomas in the Elderly: Diagnosis and Treatment of the Great Neurological ImitatorRegina PhilyriaNessuna valutazione finora
- UGIBDocumento5 pagineUGIBdwyane0033100% (1)
- Esophageal Varices Diagnosis and TreatmentDocumento20 pagineEsophageal Varices Diagnosis and Treatmentx483xDNessuna valutazione finora
- B. Aortic Stenosis: DefinitionDocumento2 pagineB. Aortic Stenosis: DefinitionNichole Audrey SaavedraNessuna valutazione finora
- Stroke and Cerebrovascular DiseaseDocumento14 pagineStroke and Cerebrovascular DiseaseMarwan M.Nessuna valutazione finora
- Damage Control ResuscitationDocumento24 pagineDamage Control ResuscitationPaulShaneHerreraZorrillaNessuna valutazione finora
- Pulmonary CirculationDocumento4 paginePulmonary CirculationDr Md Abedur RahmanNessuna valutazione finora
- Toxic Megacolon: Emergency Surgery Indications for Severe ColitisDocumento10 pagineToxic Megacolon: Emergency Surgery Indications for Severe ColitisVikas MataiNessuna valutazione finora
- Management of Hyperkalaemia and HypokalaemiaDocumento21 pagineManagement of Hyperkalaemia and Hypokalaemiaferoza97Nessuna valutazione finora
- Ischemic StrokeDocumento49 pagineIschemic StrokeMirna Ayu Permata SariNessuna valutazione finora
- Nephritic/nephrotic Syndrome.Documento37 pagineNephritic/nephrotic Syndrome.Kelechi OtamiriNessuna valutazione finora
- Management of Infective EndocarditisDocumento14 pagineManagement of Infective Endocarditismhafzam2020Nessuna valutazione finora
- Acute Arterial Occlusion - FINALDocumento32 pagineAcute Arterial Occlusion - FINALNaina Dalidig Benito100% (1)
- Angina Symptoms, Causes, Tests and TreatmentDocumento33 pagineAngina Symptoms, Causes, Tests and TreatmentAnonymous mIw67bMXNessuna valutazione finora
- Blood Pressure RegulationDocumento35 pagineBlood Pressure Regulationبراءة أحمد السلاماتNessuna valutazione finora
- Cerebellar DisordersDocumento12 pagineCerebellar DisordersAnn SamNessuna valutazione finora
- Tetralogy of FallotDocumento26 pagineTetralogy of FallotGI SanadaNessuna valutazione finora
- Hemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUDocumento27 pagineHemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUAbdisalan hassanNessuna valutazione finora
- Lower Gastrointestinal BleedingDocumento18 pagineLower Gastrointestinal Bleedingosama nawaysehNessuna valutazione finora
- Acute Gastrointestinal Bleeding GuideDocumento47 pagineAcute Gastrointestinal Bleeding GuideJohn Clements Galiza100% (1)
- Complications of Myocardial InfarctionDocumento50 pagineComplications of Myocardial InfarctionAli Baker Algelane50% (2)
- Gotham City: A Study into the Darkness Reveals Dangers WithinDocumento13 pagineGotham City: A Study into the Darkness Reveals Dangers WithinajNessuna valutazione finora
- FST Handbook 2014-Final Copy 1 PDFDocumento382 pagineFST Handbook 2014-Final Copy 1 PDFDelvon DownerNessuna valutazione finora
- Convocation ProgramDocumento125 pagineConvocation ProgramZirak TayebNessuna valutazione finora
- Progibb LV Plus PGR - Low Voc FormulationDocumento2 pagineProgibb LV Plus PGR - Low Voc FormulationDodik Novie PurwantoNessuna valutazione finora
- Chapter 10 AP GP PDFDocumento3 pagineChapter 10 AP GP PDFGeorge ChooNessuna valutazione finora
- European GMP Annex 1 - 2008 Edition - 'Pmeasuring'Documento3 pagineEuropean GMP Annex 1 - 2008 Edition - 'Pmeasuring'Khairul AnwarNessuna valutazione finora
- 12 Week Heavy Slow Resistance Progression For Patellar TendinopathyDocumento4 pagine12 Week Heavy Slow Resistance Progression For Patellar TendinopathyHenrique Luís de CarvalhoNessuna valutazione finora
- Chemistry of FormazanDocumento36 pagineChemistry of FormazanEsteban ArayaNessuna valutazione finora
- Madeleine Ker - TakeoverDocumento91 pagineMadeleine Ker - Takeover66677785100% (1)
- ASA 2018 Catalog WebDocumento48 pagineASA 2018 Catalog WebglmedinaNessuna valutazione finora
- Railway Airport Docks and HarbourDocumento21 pagineRailway Airport Docks and HarbourvalarmathibalanNessuna valutazione finora
- Swami Rama's demonstration of voluntary control over autonomic functionsDocumento17 pagineSwami Rama's demonstration of voluntary control over autonomic functionsyunjana100% (1)
- Sto - Cristo Proper Integrated School 1 Grading Grade 9 Science Table of SpecializationDocumento2 pagineSto - Cristo Proper Integrated School 1 Grading Grade 9 Science Table of Specializationinah jessica valerianoNessuna valutazione finora
- 07.03.09 Chest Physiotherapy PDFDocumento9 pagine07.03.09 Chest Physiotherapy PDFRakesh KumarNessuna valutazione finora
- Canon imageFORMULA DR-X10CDocumento208 pagineCanon imageFORMULA DR-X10CYury KobzarNessuna valutazione finora
- Essentials For Professionals: Road Surveys Using SmartphonesDocumento25 pagineEssentials For Professionals: Road Surveys Using SmartphonesDoly ManurungNessuna valutazione finora
- Feline DermatologyDocumento55 pagineFeline DermatologySilviuNessuna valutazione finora
- Is.4162.1.1985 Graduated PipettesDocumento23 pagineIs.4162.1.1985 Graduated PipettesBala MuruNessuna valutazione finora
- Organizing Small Items with Glass Bottle OrganizersDocumento70 pagineOrganizing Small Items with Glass Bottle OrganizersDy SaiNessuna valutazione finora
- Elevator Traction Machine CatalogDocumento24 pagineElevator Traction Machine CatalogRafif100% (1)
- 2 - Soil-Only Landfill CoversDocumento13 pagine2 - Soil-Only Landfill Covers齐左Nessuna valutazione finora
- Crew Served WeaponsDocumento11 pagineCrew Served WeaponsKyle Fagin100% (1)
- DR-M260 User Manual ENDocumento87 pagineDR-M260 User Manual ENMasa NourNessuna valutazione finora
- Life of A Landfill PumpDocumento50 pagineLife of A Landfill PumpumidNessuna valutazione finora
- DENSO COMMON RAIL INJECTOR REPAIR GUIDEDocumento22 pagineDENSO COMMON RAIL INJECTOR REPAIR GUIDEMarcoNessuna valutazione finora
- Nikola Tesla Was Murdered by Otto Skorzeny.Documento12 pagineNikola Tesla Was Murdered by Otto Skorzeny.Jason Lamb50% (2)
- 5125 w04 Er PDFDocumento14 pagine5125 w04 Er PDFHany ElGezawyNessuna valutazione finora
- CANAL (T) Canal Soth FloridaDocumento115 pagineCANAL (T) Canal Soth FloridaMIKHA2014Nessuna valutazione finora
- WL 318 PDFDocumento199 pagineWL 318 PDFBeckty Ahmad100% (1)
- Features Integration of Differential Binomial: DX BX A X P N MDocumento4 pagineFeatures Integration of Differential Binomial: DX BX A X P N Mابو سامرNessuna valutazione finora