Potrebbero piacerti anche
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
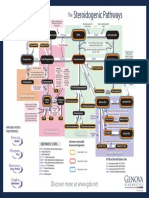
- The Steroidogenic PathwaysDocumento1 paginaThe Steroidogenic PathwaysMarkus van der WesthuizenNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Handy Summary Chart Comparing The Main Medications For PsychosisDocumento3 pagineHandy Summary Chart Comparing The Main Medications For Psychosisrowanpurdy100% (2)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Barras2.Ods 0Documento9.252 pagineBarras2.Ods 0alfredolavinNessuna valutazione finora
- EndometriosisDocumento49 pagineEndometriosisRanny0% (1)
- Anesthesia Pocket Cards 7 18 18Documento6 pagineAnesthesia Pocket Cards 7 18 18Miguel Cuevas DolotNessuna valutazione finora
- Kuis Emesis 4-MergedDocumento16 pagineKuis Emesis 4-Mergedibnu an nafisNessuna valutazione finora
- Lista 2b SiteDocumento19 pagineLista 2b SiteamocatoNessuna valutazione finora
- Anti-Fungal Drugs - Dermatology - Junior ClerkshipDocumento20 pagineAnti-Fungal Drugs - Dermatology - Junior ClerkshipRahul SrivastavaNessuna valutazione finora
- Drug StudyDocumento12 pagineDrug Studyjoaqiun100% (1)
- Case Pres Drug Study RevisionDocumento3 pagineCase Pres Drug Study RevisionJose Luis HernandezNessuna valutazione finora
- Pregnancy Category Jan.14 Ls-1Documento15 paginePregnancy Category Jan.14 Ls-1sakti_badalaNessuna valutazione finora
- Drugs Acting On Haematopoietic System of AnimalsDocumento28 pagineDrugs Acting On Haematopoietic System of AnimalsSunil100% (1)
- Pharma NotesDocumento5 paginePharma NotesyoojeongredNessuna valutazione finora
- FUNDA LEC Finals - Medication AdministrationDocumento14 pagineFUNDA LEC Finals - Medication AdministrationNel joy PaurilloNessuna valutazione finora
- PBL Parkinson'sDocumento19 paginePBL Parkinson'sPrabananthanNessuna valutazione finora
- Soft Gelatin CapsulesDocumento29 pagineSoft Gelatin CapsulesAsif KhanNessuna valutazione finora
- Gudang ObatDocumento29 pagineGudang Obatilham aceNessuna valutazione finora
- FEP Rationale TopicalCorticosteroidsDocumento5 pagineFEP Rationale TopicalCorticosteroidsJackyNessuna valutazione finora
- Drug Education Definition of TermsDocumento3 pagineDrug Education Definition of TermsLaarni EspañolaNessuna valutazione finora
- The Accidental AddictsDocumento6 pagineThe Accidental AddictsnorthandsouthnzNessuna valutazione finora
- Procedure Checklist Chapter 38, Skill 38-01: Administering IV Medication Via PRN Lock or IV LineDocumento2 pagineProcedure Checklist Chapter 38, Skill 38-01: Administering IV Medication Via PRN Lock or IV LineNursyNurseNessuna valutazione finora
- RMCD Pharmacy InventoryDocumento18 pagineRMCD Pharmacy InventoryjonjonNessuna valutazione finora
- Bioequivalence of Two Pregabalin 300 MG Capsules (Neurexal and Lyrica) in Healthy Human VolunteersDocumento5 pagineBioequivalence of Two Pregabalin 300 MG Capsules (Neurexal and Lyrica) in Healthy Human VolunteerscaturNessuna valutazione finora
- Glyburide PDFDocumento3 pagineGlyburide PDFHannaNessuna valutazione finora
- Antibiotic Policy 2014Documento32 pagineAntibiotic Policy 2014shah007zaad100% (1)
- Section1 PrescriptionwritingDocumento23 pagineSection1 PrescriptionwritingAnurag SrivastavaNessuna valutazione finora
- Dicynone InjectionDocumento3 pagineDicynone InjectionAhmed Ebid100% (2)
- Table-5 - SAE Form - 7dec22Documento5 pagineTable-5 - SAE Form - 7dec22Avinash AviNessuna valutazione finora
- Freudenreich - PsychopharmUpdate 2020 - New Treatments For Schizophrenia - FINALFINAL 1 25Documento25 pagineFreudenreich - PsychopharmUpdate 2020 - New Treatments For Schizophrenia - FINALFINAL 1 25olivukovicNessuna valutazione finora
- PRINSIP TERAPI PADA PASIEN GERIATRI - Dr. Fita Rahmawati, SP - FRSDocumento60 paginePRINSIP TERAPI PADA PASIEN GERIATRI - Dr. Fita Rahmawati, SP - FRSLhyNa AiNun SofiaNessuna valutazione finora