Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- FEU NRMF Admission FormDocumento2 pagineFEU NRMF Admission FormMea Faye DinoNessuna valutazione finora
- Maternal and Child Health NursingDocumento2 pagineMaternal and Child Health NursingErika DellosaNessuna valutazione finora
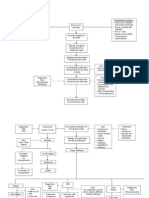
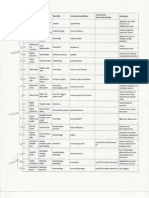
- Pathophysiology of ALL DiagramDocumento3 paginePathophysiology of ALL DiagramErika DellosaNessuna valutazione finora
- Falls in ElderlyDocumento8 pagineFalls in ElderlyErika DellosaNessuna valutazione finora
- Professional Regulatory Board of Nursing: The "Commision"Documento15 pagineProfessional Regulatory Board of Nursing: The "Commision"Erika DellosaNessuna valutazione finora
- Professional Regulatory Board of Nursing: The "Commision"Documento15 pagineProfessional Regulatory Board of Nursing: The "Commision"Erika DellosaNessuna valutazione finora
- CA ReportDocumento20 pagineCA ReportErika DellosaNessuna valutazione finora
- Med SchoolsDocumento2 pagineMed SchoolsErika DellosaNessuna valutazione finora
- Renal DisordersDocumento24 pagineRenal DisordersErika Dellosa100% (2)
- PsychDocumento23 paginePsychErika DellosaNessuna valutazione finora
- Orem Nursing TheoryDocumento2 pagineOrem Nursing TheoryErika DellosaNessuna valutazione finora
- SYPHILIS Annual TechDocumento41 pagineSYPHILIS Annual TechkimotosanNessuna valutazione finora
- Clinical Pathology and Medical Laboratory: Indonesian Journal ofDocumento6 pagineClinical Pathology and Medical Laboratory: Indonesian Journal ofIma PratiwiNessuna valutazione finora
- Dental Management of The Patient With HIVAIDS 2002Documento6 pagineDental Management of The Patient With HIVAIDS 2002drkameshNessuna valutazione finora
- John CarnevaleDocumento8 pagineJohn Carnevaleapi-209693106Nessuna valutazione finora
- Vector ControlDocumento11 pagineVector ControlMayuri Vohra100% (1)
- The National Health SituationDocumento167 pagineThe National Health SituationCes AriaNessuna valutazione finora
- Imci Chart Booklet Up DateDocumento6 pagineImci Chart Booklet Up DateifyejinkeonyeNessuna valutazione finora
- Syllabus Hiv AidsDocumento3 pagineSyllabus Hiv Aidsniketut alit arminiNessuna valutazione finora
- Antifungal AntibioticsDocumento16 pagineAntifungal AntibioticsLyadelou FortuNessuna valutazione finora
- Standard Operating Procedures Manual For The Management of TheDocumento114 pagineStandard Operating Procedures Manual For The Management of TheHarry GaiyaNessuna valutazione finora
- An Accident With A Gates Glidden Drill in Endodontic PracticeDocumento2 pagineAn Accident With A Gates Glidden Drill in Endodontic PracticeahujasurajNessuna valutazione finora
- Dermatology Written Exam 2007Documento6 pagineDermatology Written Exam 2007Abdullah Matar BadranNessuna valutazione finora
- Bisexual Invisibility:: Impacts and RecommendationsDocumento47 pagineBisexual Invisibility:: Impacts and RecommendationsprideinutahNessuna valutazione finora
- Family Life, Reproductive Health, and Population Education:: Information Series On School HealthDocumento90 pagineFamily Life, Reproductive Health, and Population Education:: Information Series On School HealthChris McIverNessuna valutazione finora
- Cambridge A As Level Biology Mark Scheme 2 Winter 2007Documento5 pagineCambridge A As Level Biology Mark Scheme 2 Winter 2007rasNessuna valutazione finora
- Bpjs NovemberDocumento219 pagineBpjs NovemberAnonymous KSvPjR2DNessuna valutazione finora
- Plot 126, Solent Avenue, Tel: (+256) 771256301 Mbuya, Kampala, Uganda P. O. Box 8379Documento7 paginePlot 126, Solent Avenue, Tel: (+256) 771256301 Mbuya, Kampala, Uganda P. O. Box 8379George LumiisaNessuna valutazione finora
- Pictures of Six Sexual Transmitted InfectionDocumento6 paginePictures of Six Sexual Transmitted InfectionDavia ColmanNessuna valutazione finora
- Health Is Very Important in Our Daily LivesDocumento2 pagineHealth Is Very Important in Our Daily LivesFit RINessuna valutazione finora
- The Miracle of Q RAK CultivationDocumento308 pagineThe Miracle of Q RAK CultivationRafyta100% (4)
- Internship Plan Surakshya Karki University of North Carolina GreensboroDocumento13 pagineInternship Plan Surakshya Karki University of North Carolina Greensboroapi-310446292Nessuna valutazione finora
- HIV Related Policies and Guidelines Issuances: Training On HIV Counseling and Testing and Facility-Based HIV ScreeningDocumento77 pagineHIV Related Policies and Guidelines Issuances: Training On HIV Counseling and Testing and Facility-Based HIV ScreeningJovania B.Nessuna valutazione finora
- NSTP Project ProposalDocumento3 pagineNSTP Project ProposalIris FuedanNessuna valutazione finora
- NYCAHN Is Now VOCAL New York!Documento3 pagineNYCAHN Is Now VOCAL New York!VOCAL-NYNessuna valutazione finora
- An Approach To Fever Throught Boger BoenninghausenDocumento10 pagineAn Approach To Fever Throught Boger BoenninghausenHomoeopathic Pulse100% (2)
- Pregestational ConditionsDocumento46 paginePregestational ConditionsSheryl M. Ablao50% (2)
- Chronic Viral HepatitisDocumento66 pagineChronic Viral HepatitisSuresh KadliNessuna valutazione finora
- Annual Report 2009 10Documento189 pagineAnnual Report 2009 10tkhalifaNessuna valutazione finora
- History OsteomielitisDocumento4 pagineHistory OsteomielitisMuhammad Hamka Maha PutraNessuna valutazione finora
- Ppg-Gdch-Nur-53 Abbreviations and SymbolsDocumento13 paginePpg-Gdch-Nur-53 Abbreviations and SymbolsKenny JosefNessuna valutazione finora