Potrebbero piacerti anche
- Estimated Blood Loss in Craniotomy: Diana Sitohang, Rachmawati AM, Mansyur ArifDocumento3 pagineEstimated Blood Loss in Craniotomy: Diana Sitohang, Rachmawati AM, Mansyur ArifJihadatul KholilahNessuna valutazione finora
- Lab HemostasisDocumento29 pagineLab HemostasisTingLi Lucia Lorigiano100% (2)
- Strategies For Improving Visualization During Endoscopic Skull Base SurgeryDocumento10 pagineStrategies For Improving Visualization During Endoscopic Skull Base SurgeryTi FaNessuna valutazione finora
- Blood TransfusionDocumento11 pagineBlood Transfusionsaid tariqNessuna valutazione finora
- 7: Effective Transfusion in Surgery and Critical CareDocumento16 pagine7: Effective Transfusion in Surgery and Critical CareNick-Hugh Sean WisdomNessuna valutazione finora
- Blood SmearDocumento7 pagineBlood SmearMarice Ferrufino SchmidtNessuna valutazione finora
- Best Practices of Apheresis in Hematopoietic Cell TransplantationDa EverandBest Practices of Apheresis in Hematopoietic Cell TransplantationSyed A. AbutalibNessuna valutazione finora
- Transfusión IntraoperatoriaDocumento24 pagineTransfusión IntraoperatoriaGiovany Salinas100% (1)
- A Compendium of Tranfusion Prectice Guidelines ARC Edition 4.0 Jan 2021Documento75 pagineA Compendium of Tranfusion Prectice Guidelines ARC Edition 4.0 Jan 2021H Stuard B CocNessuna valutazione finora
- Guia CIRSEDocumento14 pagineGuia CIRSEjfayalaNessuna valutazione finora
- Massive Tranfusion Protocol: Oleh ErtigaDocumento13 pagineMassive Tranfusion Protocol: Oleh ErtigaAnonymous BQM9271ZXNessuna valutazione finora
- Avian Blood Collection and Hematology - WSAVA 2015 Congress - VINDocumento4 pagineAvian Blood Collection and Hematology - WSAVA 2015 Congress - VINMustafa AL-AsadsyNessuna valutazione finora
- Blood Consumption in Total Arterial Coronary Artery Bypass GraftingDocumento16 pagineBlood Consumption in Total Arterial Coronary Artery Bypass Graftinginfo sekolahNessuna valutazione finora
- PBM (Autosaved)Documento36 paginePBM (Autosaved)dr AmitNessuna valutazione finora
- Safety and Ef Ficacy of An Endovascular-First Approach To Acute Limb IschemiaDocumento9 pagineSafety and Ef Ficacy of An Endovascular-First Approach To Acute Limb IschemiaSisca Dwi AgustinaNessuna valutazione finora
- Blood Bank ManualDocumento29 pagineBlood Bank ManualMarice Ferrufino SchmidtNessuna valutazione finora
- Gupea 2077 69251 1.pdf JsessionidDocumento48 pagineGupea 2077 69251 1.pdf JsessionidАнастасияNessuna valutazione finora
- Cost-Effectiveness of Blood Transfusion and White Cell Reduction in Elective Colorectal SurgeryDocumento4 pagineCost-Effectiveness of Blood Transfusion and White Cell Reduction in Elective Colorectal Surgerymy accountNessuna valutazione finora
- IndianJAnaesth563234-2277078 061930Documento4 pagineIndianJAnaesth563234-2277078 061930Eka SetiyaniNessuna valutazione finora
- Comparing A Non-Invasive Hemodynamic Monitor With Minimally Invasive Monitoring During Major Open Abdominal Surgery-2Documento6 pagineComparing A Non-Invasive Hemodynamic Monitor With Minimally Invasive Monitoring During Major Open Abdominal Surgery-2Nadhia KhairunnisaNessuna valutazione finora
- Tanner 2018Documento5 pagineTanner 2018Ricardo Arturo Frias RodriguezNessuna valutazione finora
- Algoritmo de Transfusion en Pacientes CardiologicosDocumento8 pagineAlgoritmo de Transfusion en Pacientes CardiologicosLyonTrioréNessuna valutazione finora
- 965 FullDocumento7 pagine965 FullRakhman FaridNessuna valutazione finora
- The Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open ReconstructionDocumento10 pagineThe Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open Reconstructiontmarrero00Nessuna valutazione finora
- Managing Coagulopathy ICUDocumento38 pagineManaging Coagulopathy ICUMirabela Colac100% (1)
- Frank 2019Documento15 pagineFrank 2019Oliver ArteagaNessuna valutazione finora
- Analysis of Blood Cross-Match Ordering Practice in Surgical Patients at Ndola Central HospitalDocumento7 pagineAnalysis of Blood Cross-Match Ordering Practice in Surgical Patients at Ndola Central HospitalCandy CarlaNessuna valutazione finora
- Bleeding TimeDocumento9 pagineBleeding TimeulumNessuna valutazione finora
- Assessment of The Utilization Patterns of Blood AT Mazabuka General Hospital, ZambiaDocumento11 pagineAssessment of The Utilization Patterns of Blood AT Mazabuka General Hospital, ZambiaMukale Chipego MoongaNessuna valutazione finora
- Assessment of The Utilization Patterns of Blood AT Mazabuka General Hospital, ZambiaDocumento11 pagineAssessment of The Utilization Patterns of Blood AT Mazabuka General Hospital, ZambiaMukale Chipego MoongaNessuna valutazione finora
- Leaflet Asam UratDocumento9 pagineLeaflet Asam UratParisha IchaNessuna valutazione finora
- MSBOS PrithvirajDocumento8 pagineMSBOS Prithvirajkarun1889Nessuna valutazione finora
- Arteriovenous Thrombosis in Chronic Renal Failure Patients Receiving Renal Replacement TherapyDocumento6 pagineArteriovenous Thrombosis in Chronic Renal Failure Patients Receiving Renal Replacement TherapyMaya RustamNessuna valutazione finora
- Thromboelastography (TEG) and Rotational Thromboelastometry (ROTEM) : Applications in AnesthesiaDocumento25 pagineThromboelastography (TEG) and Rotational Thromboelastometry (ROTEM) : Applications in AnesthesiaDiana PredenciucNessuna valutazione finora
- Acute Limb Ischemic: Divisi Bedah Vaskular Melfrits R Siwabessy, MDDocumento26 pagineAcute Limb Ischemic: Divisi Bedah Vaskular Melfrits R Siwabessy, MDMelfrits SiwabessyNessuna valutazione finora
- Transfusion Guidelines HemDocumento4 pagineTransfusion Guidelines HemnandhinisankaranNessuna valutazione finora
- Transcatheter Aortic Valve Replacement: A How-to Guide for Cardiologists and Cardiac SurgeonsDa EverandTranscatheter Aortic Valve Replacement: A How-to Guide for Cardiologists and Cardiac SurgeonsNessuna valutazione finora
- Specialised Vascular Services Service Specification AdultsDocumento25 pagineSpecialised Vascular Services Service Specification AdultsDr-Iyad AljuaidiNessuna valutazione finora
- Dietrich 2005Documento8 pagineDietrich 2005my accountNessuna valutazione finora
- A-Line Complication PDFDocumento8 pagineA-Line Complication PDFaeagesNessuna valutazione finora
- Blood Wastage in A Tertiary Hospital Laboratory in Tacloban CityDocumento25 pagineBlood Wastage in A Tertiary Hospital Laboratory in Tacloban CityralfNessuna valutazione finora
- Antiplatelet Drugs: Mechanisms and Risks of Bleeding Following Cardiac OperationsDocumento18 pagineAntiplatelet Drugs: Mechanisms and Risks of Bleeding Following Cardiac OperationsViona PrasetyoNessuna valutazione finora
- 6.6) Diagnostic and Therapeutic Abdominal Paracentesis - UpToDateDocumento18 pagine6.6) Diagnostic and Therapeutic Abdominal Paracentesis - UpToDatefedericoNessuna valutazione finora
- Platelet Counting by The Coulter LH 750, Sysmex XE 2100Documento7 paginePlatelet Counting by The Coulter LH 750, Sysmex XE 2100blanket_thNessuna valutazione finora
- Determining Severe GI BleedDocumento8 pagineDetermining Severe GI BleedDanny SilvaNessuna valutazione finora
- Journal of Dental Research: Blood Loss in Oral SurgeryDocumento11 pagineJournal of Dental Research: Blood Loss in Oral SurgeryFerdina NidyasariNessuna valutazione finora
- Review Article: Computed Tomography in The Evaluation For Transcatheter Aortic Valve Implantation (TAVI)Documento13 pagineReview Article: Computed Tomography in The Evaluation For Transcatheter Aortic Valve Implantation (TAVI)Paul SchoenhagenNessuna valutazione finora
- Anesthesiology 2015Documento11 pagineAnesthesiology 2015The Vancouver SunNessuna valutazione finora
- Tavr: TaviDocumento3 pagineTavr: TaviPaul SchoenhagenNessuna valutazione finora
- Jurnal THTDocumento3 pagineJurnal THTValentina AdindaNessuna valutazione finora
- Addison K May, MD John P Reilly, MD, Msce Scott Manaker, MD, PHD Arthur J Silvergleid, MD Geraldine Finlay, MD Contributor DisclosuresDocumento12 pagineAddison K May, MD John P Reilly, MD, Msce Scott Manaker, MD, PHD Arthur J Silvergleid, MD Geraldine Finlay, MD Contributor DisclosuresAlvaro HaroNessuna valutazione finora
- Trends in The Prevalence and Outcomes of Radial and Femoral Approaches To Percutaneous Coronary InterventionDocumento8 pagineTrends in The Prevalence and Outcomes of Radial and Femoral Approaches To Percutaneous Coronary InterventionYashinta MaharaniNessuna valutazione finora
- Blood Transfusion - Indications, Administration and Adverse Reactions PDFDocumento9 pagineBlood Transfusion - Indications, Administration and Adverse Reactions PDFStacey WoodsNessuna valutazione finora
- Use of Blood Products in The Critically IllDocumento25 pagineUse of Blood Products in The Critically IllAna María Díaz MedinaNessuna valutazione finora
- Practice Guidelines For Perioperative Blood Management An Updated Report by The American Society of Anesthesiologists Task Force OnDocumento13 paginePractice Guidelines For Perioperative Blood Management An Updated Report by The American Society of Anesthesiologists Task Force OnMadalina TalpauNessuna valutazione finora
- Arterio-Venous Fistula Recirculation in Hemodialysis: Causes and PrevalencesDocumento8 pagineArterio-Venous Fistula Recirculation in Hemodialysis: Causes and PrevalencesMashiur RahmanNessuna valutazione finora
- Annsurg00185 0122Documento6 pagineAnnsurg00185 0122Fajr MuzammilNessuna valutazione finora
- AutotransfusionDocumento5 pagineAutotransfusionydtrgnNessuna valutazione finora
- Blood Group ConferenceDocumento7 pagineBlood Group Conferencemahi mNessuna valutazione finora
- Accessory TragusDocumento3 pagineAccessory TragusDeba P SarmaNessuna valutazione finora
- Acantholytic Dermatosis With DyskeratosisDocumento11 pagineAcantholytic Dermatosis With DyskeratosisDeba P SarmaNessuna valutazione finora
- Pilar Cyst With CrystalsDocumento2 paginePilar Cyst With CrystalsDeba P SarmaNessuna valutazione finora
- Acantholytic Solar Keratosis, M 67, Forehead PDFDocumento6 pagineAcantholytic Solar Keratosis, M 67, Forehead PDFDeba P SarmaNessuna valutazione finora
- Acantholytic Bullous DiseaseDocumento4 pagineAcantholytic Bullous DiseaseDeba P SarmaNessuna valutazione finora
- Acantholytic Actinic KeratosisDocumento4 pagineAcantholytic Actinic KeratosisDeba P SarmaNessuna valutazione finora
- Acantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Documento3 pagineAcantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Deba P SarmaNessuna valutazione finora
- Xanthogranuloma PPT DSDocumento9 pagineXanthogranuloma PPT DSDeba P SarmaNessuna valutazione finora
- Acantholytic Acanthoma. M 60, ScrotumDocumento8 pagineAcantholytic Acanthoma. M 60, ScrotumDeba P SarmaNessuna valutazione finora
- Results of Search in Google Scholar On 'Deba P Sarma'Documento28 pagineResults of Search in Google Scholar On 'Deba P Sarma'Deba P SarmaNessuna valutazione finora
- Balanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Documento6 pagineBalanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Deba P SarmaNessuna valutazione finora
- Xanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDocumento7 pagineXanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDeba P SarmaNessuna valutazione finora
- Xanthogranuloma, M 30, Right ElbowDocumento4 pagineXanthogranuloma, M 30, Right ElbowDeba P SarmaNessuna valutazione finora
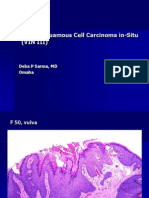
- Vulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDocumento6 pagineVulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDeba P SarmaNessuna valutazione finora
- Verrucous Epidermal Nevus. F 43, ScalpDocumento4 pagineVerrucous Epidermal Nevus. F 43, ScalpDeba P SarmaNessuna valutazione finora
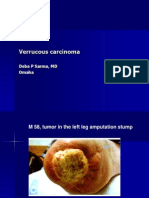
- Verrucous Carcinoma., M 58, Left Leg Amputation StumpDocumento7 pagineVerrucous Carcinoma., M 58, Left Leg Amputation StumpDeba P SarmaNessuna valutazione finora
- Verrucous Carcinoma of The Foot, M 63, Left FootDocumento8 pagineVerrucous Carcinoma of The Foot, M 63, Left FootDeba P Sarma100% (1)
- Verruca Vulgaris., M 22.,PPTDocumento2 pagineVerruca Vulgaris., M 22.,PPTDeba P SarmaNessuna valutazione finora
- Swedish Medical Center Patient LetterDocumento2 pagineSwedish Medical Center Patient LetterMichael_Lee_RobertsNessuna valutazione finora
- Final-Exam Neurosurgery - 3-VersionDocumento6 pagineFinal-Exam Neurosurgery - 3-VersionMAMA LALANessuna valutazione finora
- Dead Space ManagementDocumento26 pagineDead Space ManagementIgnasNessuna valutazione finora
- Research Paper - Celiac DiseaseDocumento5 pagineResearch Paper - Celiac Diseaseapi-316625517100% (1)
- Virani Et Al 2021 Heart Disease and Stroke Statistics 2021 UpdateDocumento490 pagineVirani Et Al 2021 Heart Disease and Stroke Statistics 2021 UpdatehendridunantikoNessuna valutazione finora
- Genital ProlapseDocumento13 pagineGenital ProlapsesmbawasainiNessuna valutazione finora
- Medical Negligence in Ghana Another Look at Asantekramo 1Documento3 pagineMedical Negligence in Ghana Another Look at Asantekramo 1SAMMY100% (1)
- Care For Respiratory and Circulatory SystemsDocumento15 pagineCare For Respiratory and Circulatory SystemsJesse Kate GonzalesNessuna valutazione finora
- Aerobic and Anaerobic ExercisesDocumento3 pagineAerobic and Anaerobic ExercisesBonak na BataNessuna valutazione finora
- Problem 1 Emergency Medicine Block: Agustina Cynthia Cesari S 405140066 Group 1Documento90 pagineProblem 1 Emergency Medicine Block: Agustina Cynthia Cesari S 405140066 Group 1Astri GunardiNessuna valutazione finora
- HemostasisDocumento5 pagineHemostasisPadmavathi C100% (1)
- Social Change Campaign in IndiaDocumento7 pagineSocial Change Campaign in IndiaGauri GargNessuna valutazione finora
- Anxiety & Related Disorders PowerPoint (19-20) PDFDocumento57 pagineAnxiety & Related Disorders PowerPoint (19-20) PDFScrew you scribdNessuna valutazione finora
- What Is DouchingDocumento8 pagineWhat Is DouchingMitch Elle InfanteNessuna valutazione finora
- BCM 299 Assessment of An Injured PatientDocumento3 pagineBCM 299 Assessment of An Injured PatientTechnoveNessuna valutazione finora
- Chief Complaints: Sl. Medicine Name Dosage Freq. Duration InstructionsDocumento4 pagineChief Complaints: Sl. Medicine Name Dosage Freq. Duration InstructionstejaminnikantiNessuna valutazione finora
- PicaDocumento10 paginePicafelinndNessuna valutazione finora
- HerniaDocumento47 pagineHerniamalathiNessuna valutazione finora
- General AnesthesiaDocumento22 pagineGeneral AnesthesiaDr Anais AsimNessuna valutazione finora
- Courtney Nance - Rad Tech Cover Letter and ResumeDocumento2 pagineCourtney Nance - Rad Tech Cover Letter and Resumeapi-282877213Nessuna valutazione finora
- Medicare Correct Coding GD PDFDocumento58 pagineMedicare Correct Coding GD PDFvrushgangNessuna valutazione finora
- Current Status of Health and Disease Burden in IndiaDocumento23 pagineCurrent Status of Health and Disease Burden in IndiaKavi rajput100% (1)
- To Study The Influence of Mandibular Exercise On Pain, Mouth Opening and Quality of Life in Post-Surgical Oral Cavity Cancer Individuals With TrismusDocumento3 pagineTo Study The Influence of Mandibular Exercise On Pain, Mouth Opening and Quality of Life in Post-Surgical Oral Cavity Cancer Individuals With TrismusInternational Educational Applied Scientific Research Journal (IEASRJ)Nessuna valutazione finora
- Design of FPDDocumento2 pagineDesign of FPDSorabh JainNessuna valutazione finora
- D Dimer Test in VTEDocumento35 pagineD Dimer Test in VTEscribmedNessuna valutazione finora
- 09 - Urinary System ReviewDocumento6 pagine09 - Urinary System ReviewDarren Atwaroo100% (1)
- Gastrocnemius Slide SurgeryDocumento2 pagineGastrocnemius Slide SurgeryHein Aung ZawNessuna valutazione finora
- Checklist MS 1 and 2Documento40 pagineChecklist MS 1 and 2mark OrpillaNessuna valutazione finora
- GTD Case StudyDocumento9 pagineGTD Case StudyZnarf Izlah Sadanreb100% (1)
- Employee HealthDocumento3 pagineEmployee HealthkrishkeshwalaNessuna valutazione finora