Potrebbero piacerti anche
- Echocardiography in ICUDa EverandEchocardiography in ICUMichel SlamaNessuna valutazione finora
- Electrocardiographic Predictors of Incident Atrial Fibrillation - DavidDocumento6 pagineElectrocardiographic Predictors of Incident Atrial Fibrillation - DavidDavid Jimmy Kurniawan RejosaputroNessuna valutazione finora
- Practice Intersection: How I Approach Thrombus in My Daily Clinical PracticeDocumento57 paginePractice Intersection: How I Approach Thrombus in My Daily Clinical PracticeSOLACI - Sociedad Latinoamericana de Cardiología IntervencionistaNessuna valutazione finora
- Cardiac Risk AssessmentsDocumento18 pagineCardiac Risk AssessmentsVane27Nessuna valutazione finora
- Facc, Fesc: Outpatient Practice Heart Center at The IsarDocumento94 pagineFacc, Fesc: Outpatient Practice Heart Center at The IsaryingubhaiNessuna valutazione finora
- Presentation CCRDocumento51 paginePresentation CCRgellerdocNessuna valutazione finora
- ST Jude DefibDocumento46 pagineST Jude DefibCorina DiaconescuNessuna valutazione finora
- Pre Op For LobectomyDocumento35 paginePre Op For LobectomyMuhammad Umer SaeedNessuna valutazione finora
- Predictive Variables For Mortality After Acute Ischemic StrokeDocumento9 paginePredictive Variables For Mortality After Acute Ischemic StrokeOscar PérezNessuna valutazione finora
- Defer Study: 5-Year Follow-UpDocumento21 pagineDefer Study: 5-Year Follow-UpVictor VacariuNessuna valutazione finora
- Abordaje Enf CarotideaDocumento57 pagineAbordaje Enf CarotideaOscar FalconNessuna valutazione finora
- Driving Pressure and Survival in ARDS-Amato-ESM-NEJM 2015Documento57 pagineDriving Pressure and Survival in ARDS-Amato-ESM-NEJM 2015SumroachNessuna valutazione finora
- 01 Ortel BRIDGEDocumento24 pagine01 Ortel BRIDGEWallnut StreetNessuna valutazione finora
- Surgery Oral Sildenafil To Control Pulmonary Hypertension After Congenital HeartDocumento7 pagineSurgery Oral Sildenafil To Control Pulmonary Hypertension After Congenital HeartYuliawati GayoNessuna valutazione finora
- Management of DVTDocumento46 pagineManagement of DVTSteven Hartanto Kurniawan50% (2)
- Cardiogenic Shock: Nick Tehrani, MD Saharman Leman Int - CardilogistDocumento54 pagineCardiogenic Shock: Nick Tehrani, MD Saharman Leman Int - CardilogistSigit_RokhmadiNessuna valutazione finora
- 400pmET Transcatheter Tricuspid Valve Treatment TCT 2019Documento22 pagine400pmET Transcatheter Tricuspid Valve Treatment TCT 2019KushanNessuna valutazione finora
- Guidelines of Implementation For The Management of Acs Focus On Coronary InterventionDocumento33 pagineGuidelines of Implementation For The Management of Acs Focus On Coronary InterventionannisNessuna valutazione finora
- Association of Multiple Infarctions and ICAS With Outcomes of Minor Stroke and TIADocumento9 pagineAssociation of Multiple Infarctions and ICAS With Outcomes of Minor Stroke and TIAJhonny Churata HuarachiNessuna valutazione finora
- Clinical, Electrocardiographic, and Echocardiographic Parameter Combination Predicts The Onset of Atrial FibrillationDocumento6 pagineClinical, Electrocardiographic, and Echocardiographic Parameter Combination Predicts The Onset of Atrial FibrillationRioNessuna valutazione finora
- Dapus 11-Anderson2004Documento6 pagineDapus 11-Anderson2004sri noviyanty yusufNessuna valutazione finora
- Treating Atrial Fibrillation Richard Schilling: ST Bartholomew's Hospital, Queen Mary's University of LondonDocumento55 pagineTreating Atrial Fibrillation Richard Schilling: ST Bartholomew's Hospital, Queen Mary's University of LondonShirakawa AlmiraNessuna valutazione finora
- Adj Her 2 SlidesDocumento37 pagineAdj Her 2 SlidesDr. Luis M. Zetina ToacheNessuna valutazione finora
- Leipsic-MDCT For TAVRDocumento58 pagineLeipsic-MDCT For TAVRLuz Dinora Sandoval CastilloNessuna valutazione finora
- Hepatopulmonary Syndrome (2014)Documento47 pagineHepatopulmonary Syndrome (2014)Robert G. Gish, MDNessuna valutazione finora
- HCV Treatment of Patients With Cirrhosis 2014 SingaporeDocumento44 pagineHCV Treatment of Patients With Cirrhosis 2014 SingaporeRobert G. Gish, MDNessuna valutazione finora
- ViewDocumento1 paginaViewmoche_raulNessuna valutazione finora
- Iacta 2011 Janak Mehta Award Winning PresentationDocumento56 pagineIacta 2011 Janak Mehta Award Winning PresentationDr.Sandeep Kumar KarNessuna valutazione finora
- T Wave Alternans For Ventricular Arrhythmia Risk StratificationDocumento5 pagineT Wave Alternans For Ventricular Arrhythmia Risk StratificationSalim VelaniNessuna valutazione finora
- 3.prof - Iman Supandiman-Prophylaxis and Treatment Thrombosis in Cancer - NewDocumento39 pagine3.prof - Iman Supandiman-Prophylaxis and Treatment Thrombosis in Cancer - NewpriyopanjiNessuna valutazione finora
- Stacom - 2019 Non Invasive Data Based or Model DrivenDocumento11 pagineStacom - 2019 Non Invasive Data Based or Model Drivennilberto2Nessuna valutazione finora
- The Femoral Arterial Access With Ultrasound Trial (FAUST)Documento20 pagineThe Femoral Arterial Access With Ultrasound Trial (FAUST)doctordocsNessuna valutazione finora
- Clinical Study Report: Open-Label, Non-Randomized, National, Multicentric, Prospective, NonDocumento4 pagineClinical Study Report: Open-Label, Non-Randomized, National, Multicentric, Prospective, NonMarius AdrianNessuna valutazione finora
- OptoxicologypresentationDocumento64 pagineOptoxicologypresentationWalaa YousefNessuna valutazione finora
- Clinical Study ReportDocumento4 pagineClinical Study ReportMarius AdrianNessuna valutazione finora
- Do We Still Need A Stethoscope - Stats For Top 10 Cardiac Tests - Roland SabbaghDocumento45 pagineDo We Still Need A Stethoscope - Stats For Top 10 Cardiac Tests - Roland SabbaghJason WongNessuna valutazione finora
- Devices Therapy For Advance HF - DR Yoga Yuniadi SPJPDocumento46 pagineDevices Therapy For Advance HF - DR Yoga Yuniadi SPJPRiska SanjayaNessuna valutazione finora
- 7.13.09 Dooley Lupus NephritisDocumento39 pagine7.13.09 Dooley Lupus NephritisTalal Ali KhanNessuna valutazione finora
- Fries PDFDocumento48 pagineFries PDFShannen Madrid TinduganNessuna valutazione finora
- Impact of High Sensitivity Troponins For 6nov Cardiac ForumDocumento39 pagineImpact of High Sensitivity Troponins For 6nov Cardiac Forummouna6685Nessuna valutazione finora
- Adult Cardiopulmonary PracticeDocumento41 pagineAdult Cardiopulmonary PracticeDinda RadetaNessuna valutazione finora
- Taxenes in Breast Cancer (Sharm)Documento76 pagineTaxenes in Breast Cancer (Sharm)safasayedNessuna valutazione finora
- AFFIRM: Atrial Fibrillation Follow-Up Investigation of Rhythm ManagementDocumento8 pagineAFFIRM: Atrial Fibrillation Follow-Up Investigation of Rhythm ManagementCiaNessuna valutazione finora
- DR Ahamad Hassan Stroke MimicsDocumento23 pagineDR Ahamad Hassan Stroke MimicskselvieNessuna valutazione finora
- Coronary Artery Bypass Graft Surgery in Patients With Ischemic Heart FailureDocumento31 pagineCoronary Artery Bypass Graft Surgery in Patients With Ischemic Heart FailureBastian SimorangkirNessuna valutazione finora
- ECG LabDocumento2 pagineECG LabMing EnNessuna valutazione finora
- Acute Limb Ischemia: A Lethal DiseaseDocumento21 pagineAcute Limb Ischemia: A Lethal Diseasekinanti deviaNessuna valutazione finora
- Coronary Artery DiseaseDocumento82 pagineCoronary Artery Diseasecortassa265Nessuna valutazione finora
- How To Perform and Interpret An Exercise TestDocumento48 pagineHow To Perform and Interpret An Exercise TestBilal AfridiNessuna valutazione finora
- Emergent Management of Acute Ischemic Stroke PDF VersionDocumento73 pagineEmergent Management of Acute Ischemic Stroke PDF VersionElizar JarNessuna valutazione finora
- Impact of Fibrinolysis On Immediate Prognosis of Patients With Out-Of-Hospital Cardiac ArrestDocumento5 pagineImpact of Fibrinolysis On Immediate Prognosis of Patients With Out-Of-Hospital Cardiac Arrestika nur annisaNessuna valutazione finora
- Acute Liver FailureDocumento31 pagineAcute Liver FailureSandyRiNessuna valutazione finora
- ARDS TrialsDocumento26 pagineARDS TrialsSwapnil PatharekarNessuna valutazione finora
- Evidence Based Medicine FinalDocumento39 pagineEvidence Based Medicine FinalNeeraj SahuNessuna valutazione finora
- Performing Exercise Treadmill TestingDocumento60 paginePerforming Exercise Treadmill Testingvera_yulia98Nessuna valutazione finora
- Guidelines For Valve QuantificationDocumento1 paginaGuidelines For Valve QuantificationZoltán Tirczka100% (1)
- Trombólisis Tromboembolia Pulmonar Dosis Media Total 2022 CartaDocumento4 pagineTrombólisis Tromboembolia Pulmonar Dosis Media Total 2022 CartaOscar BushNessuna valutazione finora
- BHD 285 - 294Documento10 pagineBHD 285 - 294nurul hidayatiNessuna valutazione finora
- Cardiocerebral Resuscitation (CCR) The New Approach To Cardiac ArrestDocumento61 pagineCardiocerebral Resuscitation (CCR) The New Approach To Cardiac ArrestLuis Prieto VegaNessuna valutazione finora
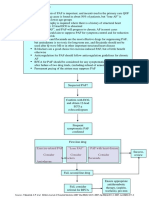
- Pathway DIAGNOSIS OF PAF FTRDocumento1 paginaPathway DIAGNOSIS OF PAF FTRYoan Eka Putra PalilingNessuna valutazione finora
- How To Read An ECGDocumento15 pagineHow To Read An ECGCFTCNessuna valutazione finora
- Percutaneous Interventional Cardiovascular Medicine - The PCR-EAPCI TextbookDocumento20 paginePercutaneous Interventional Cardiovascular Medicine - The PCR-EAPCI TextbookRanda TabbahNessuna valutazione finora
- Psycho CardiologyDocumento10 paginePsycho Cardiologyciobanusimona259970Nessuna valutazione finora
- PANCE Prep Pearls Cardio Questions PDFDocumento9 paginePANCE Prep Pearls Cardio Questions PDFkat100% (3)
- Seminar On Rheumatic Heart Disease: by Zerihun GetachewDocumento37 pagineSeminar On Rheumatic Heart Disease: by Zerihun GetachewZerihun Getachew ShiferawNessuna valutazione finora
- ECG For InternsDocumento31 pagineECG For InternsAgus SyaifudinNessuna valutazione finora
- Tachycardia Approach and ManagementDocumento41 pagineTachycardia Approach and ManagementChadi Alraies100% (5)
- CH 29 - Management of Patients With Structural, Infectious, and Inflmmatory Cardiac DisordersDocumento15 pagineCH 29 - Management of Patients With Structural, Infectious, and Inflmmatory Cardiac DisordersPye Antwan Delva100% (1)
- Kode Diagnosa PenyakitDocumento5 pagineKode Diagnosa PenyakitSelly RianiNessuna valutazione finora
- Circulationaha 110 970939Documento21 pagineCirculationaha 110 970939Michelle TedjaNessuna valutazione finora
- Athero 2 Dr. Raquid 2021Documento93 pagineAthero 2 Dr. Raquid 2021oreaNessuna valutazione finora
- ECG Made Easy - A Slow Turtle VsDocumento37 pagineECG Made Easy - A Slow Turtle VsabdallahNessuna valutazione finora
- Digoxin ToxicityDocumento9 pagineDigoxin Toxicityغيد بنت هايل بن غازي عقيل المديغم الكويكبيNessuna valutazione finora
- Cardiological Society of India Cardiology Update 2018, Kewal C. Goswami, Jaypee Bros., 1st Edition 2018 PDFDocumento1.160 pagineCardiological Society of India Cardiology Update 2018, Kewal C. Goswami, Jaypee Bros., 1st Edition 2018 PDFDana Bursacovschi100% (1)
- Unit 3 Knowledge Check 2Documento78 pagineUnit 3 Knowledge Check 2SH SNessuna valutazione finora
- Achaiki - Iatriki - April-June 2020-1Documento52 pagineAchaiki - Iatriki - April-June 2020-1NIKOLAOS SYRMOSNessuna valutazione finora
- DR AGUS SETIYANA Adult Congenital Heart Disease APDocumento25 pagineDR AGUS SETIYANA Adult Congenital Heart Disease APryandikaNessuna valutazione finora
- Gravido CardiacDocumento19 pagineGravido CardiacOUR LADY OF FATIMA UNIVERSITY COLLEGENessuna valutazione finora
- Myocardial InfarctionDocumento7 pagineMyocardial InfarctionalmiasevNessuna valutazione finora
- Atrial Flutter EmedicineDocumento8 pagineAtrial Flutter EmedicineErnis Wahyu OktianaNessuna valutazione finora
- 5 Min - PTMCDocumento28 pagine5 Min - PTMCAsim Kumar BiswasNessuna valutazione finora
- Language of Medicine 11Th Edition Chabner Test Bank Full Chapter PDFDocumento48 pagineLanguage of Medicine 11Th Edition Chabner Test Bank Full Chapter PDFgalvinegany3a72j100% (8)
- Dyspnea Cardiac Origin STPDocumento21 pagineDyspnea Cardiac Origin STPmeiliaNessuna valutazione finora
- Full Download Book Ecg in 10 Days PDFDocumento41 pagineFull Download Book Ecg in 10 Days PDFdeborah.arnaud284100% (14)
- Divine Intervention Episode 5 Cardio A Physiology1Documento18 pagineDivine Intervention Episode 5 Cardio A Physiology1Swisskelly1Nessuna valutazione finora
- Electrocardiography: The ECG: A.D. John, MD, Lee A. Fleisher, MDDocumento19 pagineElectrocardiography: The ECG: A.D. John, MD, Lee A. Fleisher, MDCésar Vásquez AguilarNessuna valutazione finora
- CARDIODocumento10 pagineCARDIOkristineNessuna valutazione finora
- Slide Master Apm CPR N AedDocumento46 pagineSlide Master Apm CPR N AedDivyaaNessuna valutazione finora
- Review Article: Management of Cardiac Tamponade After Cardiac SurgeryDocumento10 pagineReview Article: Management of Cardiac Tamponade After Cardiac SurgeryJanuar Alfred PoliNessuna valutazione finora