Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Cwu SurgeryDocumento16 pagineCwu SurgeryAslah NabilahNessuna valutazione finora
- Respiratory System-Review PathoDocumento100 pagineRespiratory System-Review PathoSadiePartington-RiopelleNessuna valutazione finora
- Brain WavesDocumento6 pagineBrain WavesDaniel MagurianuNessuna valutazione finora
- Toxic Plants in Traditional Indian Systems of Medicine: Thomas M.Walter, Gopi G.RadhaDocumento8 pagineToxic Plants in Traditional Indian Systems of Medicine: Thomas M.Walter, Gopi G.Radharajesh_rajesh_rajeshNessuna valutazione finora
- Infectious Disease ConferenceDocumento35 pagineInfectious Disease ConferenceKatrina CajigalNessuna valutazione finora
- 16corneal DegenerationsDocumento11 pagine16corneal DegenerationsmaulanaNessuna valutazione finora
- Treating Gallbladder Cancer - A Quick GuideDocumento9 pagineTreating Gallbladder Cancer - A Quick GuideSpongebob57Nessuna valutazione finora
- Stenorol® Crypto - OS - Brochure - EN - v01 - 1020 PDFDocumento2 pagineStenorol® Crypto - OS - Brochure - EN - v01 - 1020 PDFDrivailaNessuna valutazione finora
- Virtual Watcher's Class: Covid-19 N-E-W-S: Everything You Need To "Navigate" Through The New NormalDocumento27 pagineVirtual Watcher's Class: Covid-19 N-E-W-S: Everything You Need To "Navigate" Through The New NormalValerie FischerNessuna valutazione finora
- NCM 104 Indiv and FamilyDocumento123 pagineNCM 104 Indiv and FamilyJames Peter ManatadNessuna valutazione finora
- Essential, Trace, and Nonessential Ions-1Documento3 pagineEssential, Trace, and Nonessential Ions-1John AndanNessuna valutazione finora
- Endocrine System BulletsDocumento28 pagineEndocrine System Bulletswinner gift flowersNessuna valutazione finora
- An Analysis of Shakespeare's Sonnet 147Documento5 pagineAn Analysis of Shakespeare's Sonnet 147MichaelJohnDiMartinoNessuna valutazione finora
- Cdmp2015 HandbookDocumento90 pagineCdmp2015 HandbookTony NgNessuna valutazione finora
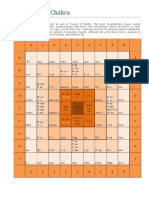
- Sarvatobhadra ChakraDocumento6 pagineSarvatobhadra Chakrasateesh_chandra_1100% (5)
- Hepatic Encephalopathy and Coma and End Stage Renal DseDocumento61 pagineHepatic Encephalopathy and Coma and End Stage Renal DseKoRnflakesNessuna valutazione finora
- 2020 Alzheimer's Disease Facts and FiguresDocumento70 pagine2020 Alzheimer's Disease Facts and Figuresprabha karanNessuna valutazione finora
- Cid en AdultosDocumento38 pagineCid en AdultosJosephGabrielNessuna valutazione finora
- PLAGUEDocumento5 paginePLAGUEHpu JogindernagerNessuna valutazione finora
- OBGYN Shelf NotesDocumento7 pagineOBGYN Shelf NotesaelteeNessuna valutazione finora
- Parkinson DiseaseDocumento10 pagineParkinson DiseaseparthibaneNessuna valutazione finora
- Insignis PCM3 Dengue, Blood Donation, HIV, Mental Health, NBS, LeprosyDocumento133 pagineInsignis PCM3 Dengue, Blood Donation, HIV, Mental Health, NBS, LeprosyNibshian Dela RosaNessuna valutazione finora
- Casestudy29 OpenabdomenDocumento14 pagineCasestudy29 Openabdomenapi-301118772100% (1)
- Chapter II Review of Related Literature and StudiesDocumento2 pagineChapter II Review of Related Literature and StudiesAnthone Manjeron70% (33)
- Coombs and Gell ClassificationDocumento34 pagineCoombs and Gell ClassificationAnamNessuna valutazione finora
- Section 2. Skin ProblemsDocumento9 pagineSection 2. Skin ProblemsAliNessuna valutazione finora
- Medical Nutrition Therapy For Cancer PreventionDocumento5 pagineMedical Nutrition Therapy For Cancer PreventionotaNessuna valutazione finora
- Vechur CowDocumento2 pagineVechur CowkappygasNessuna valutazione finora
- Case StudyDocumento12 pagineCase Studyapi-291857811Nessuna valutazione finora