Potrebbero piacerti anche
- Prostho Short NotesDocumento84 pagineProstho Short Notessamiksha100% (1)
- Delayed Eruption PDFDocumento6 pagineDelayed Eruption PDFIsharajini Prasadika Subhashni GamageNessuna valutazione finora
- 2017 2018 Dental Anatomy and Occlusion 1Documento435 pagine2017 2018 Dental Anatomy and Occlusion 1Aura UrbayoNessuna valutazione finora
- Jaw RelationshipsDocumento12 pagineJaw RelationshipsPradusha RevuruNessuna valutazione finora
- Antibiotics in Endodontics: When to Prescribe and Which Ones to UseDocumento49 pagineAntibiotics in Endodontics: When to Prescribe and Which Ones to UsemirfanulhaqNessuna valutazione finora
- Selection and Arrangement of Teeth for Complete DenturesDocumento84 pagineSelection and Arrangement of Teeth for Complete DenturesMaqbul AlamNessuna valutazione finora
- Oral Surgery in Pediatric DentistryDocumento238 pagineOral Surgery in Pediatric Dentistrydrnadeemulla khan100% (1)
- Surgical EndoDocumento16 pagineSurgical EndoTraian IlieNessuna valutazione finora
- Global DiagnosisDocumento5 pagineGlobal DiagnosisdrsmritiNessuna valutazione finora
- Tooth Form & Function - IDocumento32 pagineTooth Form & Function - IMasayi K MackatianiNessuna valutazione finora
- Module 3 - Nursing Assessment in Family Nursing PracticeDocumento7 pagineModule 3 - Nursing Assessment in Family Nursing PracticeRogedith DelaRosaNessuna valutazione finora
- Viral Hepatitis (Virus Hepatitis)Documento66 pagineViral Hepatitis (Virus Hepatitis)Ilmiah Bagus100% (1)
- Application of The Rotational Path Design Concept To A Removable Partial Denture With A Distal-Extension BaseDocumento3 pagineApplication of The Rotational Path Design Concept To A Removable Partial Denture With A Distal-Extension BaseChepe LemusNessuna valutazione finora
- Step 2-3-Clinical Checklist: Behavioral Science (8 Videos 2 Hours 9 Minutes)Documento14 pagineStep 2-3-Clinical Checklist: Behavioral Science (8 Videos 2 Hours 9 Minutes)MILTHON DAVID DIAZ PUENTES67% (3)
- Basic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionDa EverandBasic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionNessuna valutazione finora
- Concepts of Arrangement of Artifical Teeth, SelectiveDocumento7 pagineConcepts of Arrangement of Artifical Teeth, SelectiveAmar BhochhibhoyaNessuna valutazione finora
- Survey and DesignDocumento61 pagineSurvey and DesignSeena Sam100% (1)
- PhenylketonuriaDocumento10 paginePhenylketonuriaMalathy Ravendran100% (1)
- Mouth Preparation and Master Cast in Removable PartialDocumento45 pagineMouth Preparation and Master Cast in Removable PartialSrishti SrivastavaNessuna valutazione finora
- L2. Tooth Morphology and Access OpeningsDocumento6 pagineL2. Tooth Morphology and Access OpeningsUnghianu Constantin IulianNessuna valutazione finora
- Conservative Endodontics Textbooks PDFDocumento1 paginaConservative Endodontics Textbooks PDFVenkatesh Gavini0% (1)
- Acute Effects of Radiation InjuryDocumento8 pagineAcute Effects of Radiation InjuryVikas VatsNessuna valutazione finora
- Patología Bucal - Bruch (Ingles)Documento176 paginePatología Bucal - Bruch (Ingles)MarielEsmeraldaNessuna valutazione finora
- Surgical Management of Oral Pathological LesionDocumento24 pagineSurgical Management of Oral Pathological Lesionمحمد ابوالمجدNessuna valutazione finora
- Clinical Evaluation of Abutment Teeth of Removable PartialDocumento7 pagineClinical Evaluation of Abutment Teeth of Removable PartialAlex KwokNessuna valutazione finora
- Safe Injection Practices and Handling of SharpsDocumento26 pagineSafe Injection Practices and Handling of SharpsbrightyNessuna valutazione finora
- Practical Notions concerning Dental OcclusionDocumento61 paginePractical Notions concerning Dental OcclusionEmil Costruț100% (1)
- Mandibular Centricity Centric RelationDocumento3 pagineMandibular Centricity Centric RelationAmar BhochhibhoyaNessuna valutazione finora
- Seminar 2 Stomatognathic SystemDocumento41 pagineSeminar 2 Stomatognathic SystemAmit Sadhwani100% (1)
- Dentine Hypersensitivity: Developing a Person-centred Approach to Oral HealthDa EverandDentine Hypersensitivity: Developing a Person-centred Approach to Oral HealthNessuna valutazione finora
- Classification of Periodental LesionsDocumento6 pagineClassification of Periodental LesionsAsia IbraheemNessuna valutazione finora
- Class III, IV and V Composite Resin - ObjectivesDocumento4 pagineClass III, IV and V Composite Resin - ObjectivesSheena Mae OcampoNessuna valutazione finora
- SSC CROWNS: INDICATIONS & APPLICATIONDocumento24 pagineSSC CROWNS: INDICATIONS & APPLICATIONwese87Nessuna valutazione finora
- Immediate Complete Denture ProtocolDocumento2 pagineImmediate Complete Denture ProtocolFranklyn D WellsNessuna valutazione finora
- 3rd Molar Guidelines April 2021 v3Documento110 pagine3rd Molar Guidelines April 2021 v3aram meyedyNessuna valutazione finora
- Prosthodontics Section I Complete Denture Chapter 1 IntroductionDocumento12 pagineProsthodontics Section I Complete Denture Chapter 1 Introductionthenmozhi thenmozhiNessuna valutazione finora
- Managing Deep Caries LesionsDocumento5 pagineManaging Deep Caries LesionsEmeka V. ObiNessuna valutazione finora
- RPDDocumento7 pagineRPDLea TomarongNessuna valutazione finora
- ProsthoDocumento59 pagineProsthoramNessuna valutazione finora
- Ante's 1926 Law Revisited A Systematic Review On SDocumento10 pagineAnte's 1926 Law Revisited A Systematic Review On SJuan Jose Stuven RodriguezNessuna valutazione finora
- Fixed Prosthodontics II - Available Elastic Impression Materials - by Noor Al-Deen M. Al-KhanatiDocumento1 paginaFixed Prosthodontics II - Available Elastic Impression Materials - by Noor Al-Deen M. Al-KhanatiNoor Al-Deen MaherNessuna valutazione finora
- Dental Caries: Cariology - MidtermsDocumento29 pagineDental Caries: Cariology - MidtermskrstnkyslNessuna valutazione finora
- ADHESIVE BRIDGES: PRINCIPLES, PROCEDURES AND CASE REPORTDocumento22 pagineADHESIVE BRIDGES: PRINCIPLES, PROCEDURES AND CASE REPORTShekinah Andrea DumlaoNessuna valutazione finora
- Introduction to Occlusion FundamentalsDocumento33 pagineIntroduction to Occlusion FundamentalsJASPREETKAUR0410100% (1)
- Removable Prosthodontics II - Lec.7, Minor Connectors - SIUST, College of DentistyDocumento4 pagineRemovable Prosthodontics II - Lec.7, Minor Connectors - SIUST, College of DentistyNoor Al-Deen Maher0% (1)
- Latest ADA Dental Radiographic Examinations GuidelinesDocumento29 pagineLatest ADA Dental Radiographic Examinations Guidelinesjatt_mu_phattNessuna valutazione finora
- Protaper PDFDocumento5 pagineProtaper PDFWidhi Satrio NugrohoNessuna valutazione finora
- Tooth Morphology Basics: Howard Chi, D.M.DDocumento79 pagineTooth Morphology Basics: Howard Chi, D.M.DMihaela Vasiliu0% (1)
- Denture Base Design and MaterialsDocumento6 pagineDenture Base Design and MaterialsBrandon AviciiNessuna valutazione finora
- Maintaining Stability of Complete DenturesDocumento21 pagineMaintaining Stability of Complete DenturesAatish Dilip ShahNessuna valutazione finora
- Chapter 41.Ppt HypersensitivityDocumento63 pagineChapter 41.Ppt HypersensitivityMaria Mercedes LeivaNessuna valutazione finora
- !!! Root Canal Morphology and It's Relationship To Endodontic Procedures - Frank J. Vertucci !!!Documento27 pagine!!! Root Canal Morphology and It's Relationship To Endodontic Procedures - Frank J. Vertucci !!!Puscas Madalina100% (1)
- 1 s2.0 S0022391302002998 MainDocumento5 pagine1 s2.0 S0022391302002998 MainManjeev GuragainNessuna valutazione finora
- Mandibular Condylar and Subcondylar Fractures PDFDocumento16 pagineMandibular Condylar and Subcondylar Fractures PDFWayan Sutresna YasaNessuna valutazione finora
- The Art of Characterization in Dental RestorationsDocumento33 pagineThe Art of Characterization in Dental RestorationsVikas Aggarwal100% (1)
- Impressions in Fixed Partial Denture A Review UpdateDocumento5 pagineImpressions in Fixed Partial Denture A Review UpdateswapnaNessuna valutazione finora
- Direct Retainer RequirementsDocumento10 pagineDirect Retainer RequirementsAnnika Siti ResdyantiNessuna valutazione finora
- Avulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The ToothDocumento39 pagineAvulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The Toothshailesh_shenoyNessuna valutazione finora
- Management of Pediatric Mandible Fractures PDFDocumento16 pagineManagement of Pediatric Mandible Fractures PDFarfahNessuna valutazione finora
- Treating Severely Impacted Canines Through Interdisciplinary CareDocumento6 pagineTreating Severely Impacted Canines Through Interdisciplinary CareNingombam Robinson SinghNessuna valutazione finora
- CarteDocumento272 pagineCarteClaudia MoldovanuNessuna valutazione finora
- Dental Trauma Guidelines III Primary Teeth - Flores Anderson AndreassenDocumento7 pagineDental Trauma Guidelines III Primary Teeth - Flores Anderson Andreassenapi-265532519Nessuna valutazione finora
- Effect of ProTaper Universal, Endoflare, Revo-S, HyFlexDocumento3 pagineEffect of ProTaper Universal, Endoflare, Revo-S, HyFlexshamshuddin patelNessuna valutazione finora
- Dental caries classification and nomenclatureDocumento26 pagineDental caries classification and nomenclatureVinceEjorangoCabigaoNessuna valutazione finora
- Frankel 123 / Orthodontic Courses by Indian Dental AcademyDocumento41 pagineFrankel 123 / Orthodontic Courses by Indian Dental Academyindian dental academyNessuna valutazione finora
- WHO Surgical Safety ChecklistDocumento1 paginaWHO Surgical Safety ChecklistArabelle GO100% (1)
- Unit Proposal PresentationDocumento29 pagineUnit Proposal PresentationRachel CortezNessuna valutazione finora
- Kemampuan Clinical Reasoning Pada Ujian Osce Mahasiswa Kedokteran Tahun KetigaDocumento9 pagineKemampuan Clinical Reasoning Pada Ujian Osce Mahasiswa Kedokteran Tahun Ketigabelahan jiwaNessuna valutazione finora
- Commed PPT (Deepthi)Documento22 pagineCommed PPT (Deepthi)Nivedha RajanNessuna valutazione finora
- Job Title: Health and Safety OfficerDocumento3 pagineJob Title: Health and Safety OfficergiovadiNessuna valutazione finora
- Fever and RashDocumento14 pagineFever and RashwirdahajaNessuna valutazione finora
- Medicine Lec.9 - Viral Infection IIDocumento42 pagineMedicine Lec.9 - Viral Infection II7fefdfbea1Nessuna valutazione finora
- Nursing Informatics (Terminal Requirement 17)Documento1 paginaNursing Informatics (Terminal Requirement 17)Lyza MateoNessuna valutazione finora
- Argumentative Essay FinalDocumento3 pagineArgumentative Essay Finalapi-248602269Nessuna valutazione finora
- CSL AssignmentDocumento2 pagineCSL AssignmentMuhammad QubaisNessuna valutazione finora
- Occlusal Variations For Reconstructing The Natural DentitionDocumento5 pagineOcclusal Variations For Reconstructing The Natural DentitionPablo Gutiérrez Da VeneziaNessuna valutazione finora
- Periodic Health ExamDocumento23 paginePeriodic Health ExamPernel Jose Alam MicuboNessuna valutazione finora
- Enovate Biolife PortfolioDocumento8 pagineEnovate Biolife PortfolioShilpa KhadilkarNessuna valutazione finora
- Contact IsolationDocumento2 pagineContact IsolationIsworo RukmiNessuna valutazione finora
- KAC Form X Course Registration 17 and Below JUNE2022Documento5 pagineKAC Form X Course Registration 17 and Below JUNE2022ALEX SARAOSOSNessuna valutazione finora
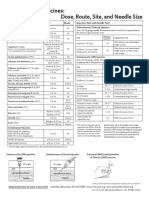
- Injection Site and Needle Size Vaccine Dose RouteDocumento1 paginaInjection Site and Needle Size Vaccine Dose RouteDr Ambana GowdaNessuna valutazione finora
- Kidney DoctorsDocumento11 pagineKidney DoctorsmamunmnNessuna valutazione finora
- Subtle Energy's Interaction W Ith The Human Body PDFDocumento18 pagineSubtle Energy's Interaction W Ith The Human Body PDFNathan JahanNessuna valutazione finora
- Bells Palsy Handbook Facial Nerve Palsy or Bells Palsy Facial Paralysis Causes, Symptoms, Treatment, Face Exercises ... (Alan MC Donald DR Alexa Smith) (Z-Library)Documento94 pagineBells Palsy Handbook Facial Nerve Palsy or Bells Palsy Facial Paralysis Causes, Symptoms, Treatment, Face Exercises ... (Alan MC Donald DR Alexa Smith) (Z-Library)mayakhoNessuna valutazione finora
- An Impression Technique For Patients With Fixed Orthodontic AppliancesDocumento2 pagineAn Impression Technique For Patients With Fixed Orthodontic Appliancesmoji_puiNessuna valutazione finora
- HospitalAdministration 2Documento13 pagineHospitalAdministration 2JairAntonAtuncarNessuna valutazione finora
- Asthease CapsuleDocumento3 pagineAsthease Capsulehk_scribdNessuna valutazione finora
- Ontario Cancer PlanDocumento64 pagineOntario Cancer PlanNetNewsLedger.comNessuna valutazione finora