Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- 6th Central Pay Commission Salary CalculatorDocumento15 pagine6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Electrician Mostly Asked MCQ For RRB ALP PDFDocumento32 pagineElectrician Mostly Asked MCQ For RRB ALP PDFSajid Faniband100% (1)
- Aci435 PDFDocumento89 pagineAci435 PDFVasanthapragash NadarajhaNessuna valutazione finora
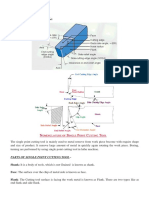
- Parts of Single Point Cutting ToolDocumento8 pagineParts of Single Point Cutting ToolMukesh sutharNessuna valutazione finora
- Mechanics of Rotor Spinning MachinesDocumento283 pagineMechanics of Rotor Spinning MachinesFelipe Melgarejo75% (4)
- MD VI Shaft DesignDocumento11 pagineMD VI Shaft DesignShatendra SahuNessuna valutazione finora
- Polyamide 610 KasarDocumento8 paginePolyamide 610 KasarAlison BurksNessuna valutazione finora
- MRI Lecture NotesDocumento33 pagineMRI Lecture NotesArungoud PoshalaNessuna valutazione finora
- 77-7 Sliding BearingDocumento11 pagine77-7 Sliding Bearingrip111176100% (1)
- Sujith - Digital Light ProcessingDocumento43 pagineSujith - Digital Light Processingapi-3827000100% (3)
- Subin S B (Virtual Keyboard)Documento36 pagineSubin S B (Virtual Keyboard)yuben josephNessuna valutazione finora
- Ushashi SMSDocumento22 pagineUshashi SMSapi-3827000Nessuna valutazione finora
- Shyam Ac Performance of Nano ElectronicsDocumento30 pagineShyam Ac Performance of Nano Electronicsapi-3827000100% (1)
- SUBIN K M Freespace Laser CommunicationsDocumento31 pagineSUBIN K M Freespace Laser Communicationsapi-3827000100% (3)
- Sreerekha (FinFET)Documento38 pagineSreerekha (FinFET)yuben josephNessuna valutazione finora
- Sreerekha (FinFET)Documento38 pagineSreerekha (FinFET)yuben josephNessuna valutazione finora
- Anand 4G WirelessDocumento31 pagineAnand 4G Wirelessapi-3827000100% (6)
- Girish TeleportationDocumento26 pagineGirish Teleportationapi-3827000100% (3)
- Sanjay - High Performance DSP ArchitecturesDocumento38 pagineSanjay - High Performance DSP Architecturesapi-3827000Nessuna valutazione finora
- Arun OFDMDocumento42 pagineArun OFDMapi-3827000Nessuna valutazione finora
- 64 Bit ComputingDocumento18 pagine64 Bit ComputingAshish MadaanNessuna valutazione finora
- Quadrics Interconnection NetworkDocumento24 pagineQuadrics Interconnection Networkapi-3827000100% (1)
- Voice MorphingDocumento31 pagineVoice Morphingapi-382700092% (13)
- Prasanna (Code Division Duplex Ing)Documento30 paginePrasanna (Code Division Duplex Ing)yuben josephNessuna valutazione finora
- Wireless FidelityDocumento22 pagineWireless Fidelitymuraliraj_sNessuna valutazione finora
- Wireless Local LoopDocumento8 pagineWireless Local Loopapi-3827000100% (1)
- Surround SystemsDocumento24 pagineSurround Systemsapi-3827000Nessuna valutazione finora
- Tele ImmersionDocumento20 pagineTele Immersionapi-3827000100% (8)
- Polymer MemoryDocumento27 paginePolymer Memoryapi-3827000100% (4)
- ProblemsDocumento32 pagineProblemsjosiedabatosNessuna valutazione finora
- AngularDocumento57 pagineAngularThomas Edoche EdocheNessuna valutazione finora
- 3 Marks PDFDocumento62 pagine3 Marks PDFNithin Aadhav.SNessuna valutazione finora
- Lecture 03Documento25 pagineLecture 03Magdalena SiahaanNessuna valutazione finora
- Classical Field TheoryDocumento35 pagineClassical Field TheorySagar JCNessuna valutazione finora
- Miniature Aluminum Electrolytic Capacitors: SeriesDocumento7 pagineMiniature Aluminum Electrolytic Capacitors: SeriesLaurentiu IacobNessuna valutazione finora
- ASCO 327 Solenoid Valves ATEX IECEx Certified For Hazardous Areas2Documento4 pagineASCO 327 Solenoid Valves ATEX IECEx Certified For Hazardous Areas2harishNessuna valutazione finora
- Higgs Lecture NotesDocumento48 pagineHiggs Lecture Noteszcapg17Nessuna valutazione finora
- ChainDocumento2 pagineChainmyusuf_engineerNessuna valutazione finora
- Effect of Structure-Directing Agent On AlPO4-n Synthesis From Aluminum DrossDocumento5 pagineEffect of Structure-Directing Agent On AlPO4-n Synthesis From Aluminum DrossXantos YulianNessuna valutazione finora
- 4 - Rate Laws and Stoichiometry - StuDocumento62 pagine4 - Rate Laws and Stoichiometry - StuTiệp MatícNessuna valutazione finora
- Drying Introduction, DefinationDocumento15 pagineDrying Introduction, DefinationChintan ModiNessuna valutazione finora
- Effect of Fly Ash and Silica Fume On Concrete": Submitted byDocumento19 pagineEffect of Fly Ash and Silica Fume On Concrete": Submitted bysushil kumarNessuna valutazione finora
- Engg Mechanics Question Bank UNIT-1Documento10 pagineEngg Mechanics Question Bank UNIT-1Thiyagarajan GurusamyNessuna valutazione finora
- MAAE 3202 Mid Term Assignment 2014Documento11 pagineMAAE 3202 Mid Term Assignment 2014Moustafa SohdyNessuna valutazione finora
- Pharmaceutical Chemistry Answer Key Blue PacopDocumento30 paginePharmaceutical Chemistry Answer Key Blue PacopJeannie UyNessuna valutazione finora
- 1-7 Manufacturing BasicsDocumento29 pagine1-7 Manufacturing BasicsFaNg KupthammasarnNessuna valutazione finora
- VibrationDocumento15 pagineVibrationCma WeyhNessuna valutazione finora
- Part 32 Welding RelatedDocumento8 paginePart 32 Welding Relatedravindra_jivaniNessuna valutazione finora
- Chemistry Form Three Q&a1Documento110 pagineChemistry Form Three Q&a1MajaningumbaoNessuna valutazione finora
- 83 WorksheetDocumento2 pagine83 WorksheetRishabh DhaulakhandiNessuna valutazione finora
- Mini Projek Meriam BuluhDocumento6 pagineMini Projek Meriam BuluheizharNessuna valutazione finora