Potrebbero piacerti anche
- Melanocytic TumorsDocumento254 pagineMelanocytic TumorsmixandgoNessuna valutazione finora
- Hemangiomas, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandHemangiomas, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Derma NotesDocumento52 pagineDerma NotesUsmanNessuna valutazione finora
- Dermatology Notes for Medical StudentsDa EverandDermatology Notes for Medical StudentsValutazione: 4 su 5 stelle4/5 (5)
- 5 - Differential Diagnosis of DermatologyDocumento6 pagine5 - Differential Diagnosis of DermatologyAyaa YousefNessuna valutazione finora
- Efflorescence of The Skin Lesions: Dr. M. Izazi HP, SP - KKDocumento40 pagineEfflorescence of The Skin Lesions: Dr. M. Izazi HP, SP - KKSaputra Tri NopiantoNessuna valutazione finora
- Dermatology - LoveDocumento433 pagineDermatology - LoveAntonio EscobarNessuna valutazione finora
- Dokumen - Pub Bedside Techniques Methods of Clinical Examination Fifth 2019nbsped 9789696375258Documento234 pagineDokumen - Pub Bedside Techniques Methods of Clinical Examination Fifth 2019nbsped 9789696375258doyoumatterindeedNessuna valutazione finora
- CME Examination DermatologyDocumento25 pagineCME Examination DermatologylimeddyNessuna valutazione finora
- Dermatology Questions and AnsDocumento147 pagineDermatology Questions and AnsEl FaroukNessuna valutazione finora
- An Approach To The Patient With ErythrodermaDocumento42 pagineAn Approach To The Patient With ErythrodermaShakilNessuna valutazione finora
- 7 Bleeding Disorders DR - AlaaDocumento35 pagine7 Bleeding Disorders DR - Alaaaj1998ajNessuna valutazione finora
- Paraneoplastic DermatosesDocumento57 pagineParaneoplastic DermatosesMohamed Riyaz100% (1)
- Melanocytic TumorsDocumento170 pagineMelanocytic TumorsOlteanu Dragos-Nicolae100% (1)
- Sqweqwesf Erwrewfsdfs Adasd Dhe: Dermnet NZDocumento19 pagineSqweqwesf Erwrewfsdfs Adasd Dhe: Dermnet NZkdwazirNessuna valutazione finora
- Dermnet NZ: Special Stains and TestsDocumento4 pagineDermnet NZ: Special Stains and TestsRaja Sekaran DuraiNessuna valutazione finora
- Phototherapy For Dermatologic ConditionsDocumento18 paginePhototherapy For Dermatologic ConditionsSeth MosebyNessuna valutazione finora
- Clinical Cases in Dermatology Modern Management of Acne Actinic Keratosis and Atopic DermatitisDocumento7 pagineClinical Cases in Dermatology Modern Management of Acne Actinic Keratosis and Atopic DermatitisJpratoNessuna valutazione finora
- Derma MegatableDocumento21 pagineDerma MegatableNicole ChanNessuna valutazione finora
- Dermatology OSCE Pictures 1Documento208 pagineDermatology OSCE Pictures 1medt80Nessuna valutazione finora
- Introduction To Dermatology Assessment of A Dermatologic PatientDocumento86 pagineIntroduction To Dermatology Assessment of A Dermatologic PatientAtifNessuna valutazione finora
- PediatricsDocumento38 paginePediatricskhanNessuna valutazione finora
- Oral Dermatology: Important Oral Questions & AnswersDocumento29 pagineOral Dermatology: Important Oral Questions & AnswersMedo JTNessuna valutazione finora
- Omalizumab in DermatologyDocumento35 pagineOmalizumab in DermatologyDeval MistryNessuna valutazione finora
- Distribution of Lesion: - Examination of The SkinDocumento5 pagineDistribution of Lesion: - Examination of The SkinAnanta WinartoNessuna valutazione finora
- Dermatology FinalDocumento16 pagineDermatology FinalMelinda100% (2)
- June 2022 - Dermatology - 10 McqsDocumento8 pagineJune 2022 - Dermatology - 10 McqsAhmed ShihataNessuna valutazione finora
- Self Assessment CasesDocumento512 pagineSelf Assessment CasesmixandgoNessuna valutazione finora
- Photodermatologic Disorders (Photodermatoses) : Mikias Woldetensay Dermatology & Venereology Oct 2021Documento59 paginePhotodermatologic Disorders (Photodermatoses) : Mikias Woldetensay Dermatology & Venereology Oct 2021CHALIE MEQUNessuna valutazione finora
- Emergency Dermatology: Case 1, Question 1 The Most Likely Diagnosis Is: Case 1, Question 1 The Most Likely Diagnosis IsDocumento16 pagineEmergency Dermatology: Case 1, Question 1 The Most Likely Diagnosis Is: Case 1, Question 1 The Most Likely Diagnosis IskarbikashNessuna valutazione finora
- Derm - Monitoring Systemic MedicationsDocumento3 pagineDerm - Monitoring Systemic MedicationsriskhakovNessuna valutazione finora
- Tumours of Skin: DR F Bhatti Pennine VTS Sept 08Documento39 pagineTumours of Skin: DR F Bhatti Pennine VTS Sept 08pfxbkNessuna valutazione finora
- Final Dermatology ExamDocumento37 pagineFinal Dermatology ExamheshamNessuna valutazione finora
- Dermatology SlidesDocumento16 pagineDermatology SlidesmuhammadridhwanNessuna valutazione finora
- Mnemonics in DermatologyDocumento2 pagineMnemonics in DermatologyShree ShresthaNessuna valutazione finora
- Hair Growth Disorders N Pigmentary DisordersDocumento7 pagineHair Growth Disorders N Pigmentary Disordersmrosaregina michelleNessuna valutazione finora
- Systemic Manifestations of Skin DisordersDocumento41 pagineSystemic Manifestations of Skin DisordersMeighalah ArumugamNessuna valutazione finora
- Skin Manifestations of HIV DiseaseDocumento31 pagineSkin Manifestations of HIV Diseaselovelots1234Nessuna valutazione finora
- Dermatology PDFDocumento23 pagineDermatology PDFjonyNessuna valutazione finora
- KEY: Certain, Pretty Sure, Possible: 18 Years Old/female CameDocumento8 pagineKEY: Certain, Pretty Sure, Possible: 18 Years Old/female Camefairodz salapudinNessuna valutazione finora
- Yeung H Et Al 2012. Patient Reported Reasons For The Discontinuation of Commonly Used Treatments For Moderate To Severe PsoriasisDocumento9 pagineYeung H Et Al 2012. Patient Reported Reasons For The Discontinuation of Commonly Used Treatments For Moderate To Severe PsoriasisAndi MarsaliNessuna valutazione finora
- Topical Antibiotics in DermatologyDocumento19 pagineTopical Antibiotics in DermatologyJejem Marandra EmkamasNessuna valutazione finora
- CLINICAL DERMATOLOGY (NXPowerLite)Documento119 pagineCLINICAL DERMATOLOGY (NXPowerLite)api-3710926Nessuna valutazione finora
- DermatoscopieDocumento220 pagineDermatoscopiepodacclaudiu100% (2)
- Clinical Dermatology: Carmen I Farid. MDDocumento81 pagineClinical Dermatology: Carmen I Farid. MDBahaa ShaabanNessuna valutazione finora
- Connective Tissue DiseasesDocumento54 pagineConnective Tissue DiseasesRatnakar KamathNessuna valutazione finora
- Guidelines For The Management of Nappy RashDocumento13 pagineGuidelines For The Management of Nappy RashOva PradiptaNessuna valutazione finora
- 3b Dermatology PresentationDocumento73 pagine3b Dermatology PresentationOlivia Genevieve El JassarNessuna valutazione finora
- Dermatology Skin in Systemic DiseaseDocumento47 pagineDermatology Skin in Systemic DiseaseNariska CooperNessuna valutazione finora
- Malignant Melanoma Research PaperDocumento10 pagineMalignant Melanoma Research Paperapi-272931142Nessuna valutazione finora
- Dermatology Board Review 2007 Part 3Documento42 pagineDermatology Board Review 2007 Part 3hifuka100% (1)
- Ichthyosis - Fitzpatrick Dermatology 9th EdDocumento26 pagineIchthyosis - Fitzpatrick Dermatology 9th EdIza Singson-CristobalNessuna valutazione finora
- Subungual MelanomaDocumento50 pagineSubungual Melanomastefani83Nessuna valutazione finora
- Dermatology Lectures JRRMMCDocumento10 pagineDermatology Lectures JRRMMCGi Em100% (1)
- All in OneDocumento193 pagineAll in Oneprashant singhNessuna valutazione finora
- 0 Basic Principles of DermatologyDocumento42 pagine0 Basic Principles of Dermatologymusatii100% (1)
- Dermatology Quiz 2015 AnswersDocumento40 pagineDermatology Quiz 2015 Answerspoorva shahNessuna valutazione finora
- Dermatology For The NonDermDocumento7 pagineDermatology For The NonDermDanielleNessuna valutazione finora
- Dermatopathology Patterns-2Documento38 pagineDermatopathology Patterns-2Deba P SarmaNessuna valutazione finora
- Normal Sizes and Other Aids (Radiology)Documento16 pagineNormal Sizes and Other Aids (Radiology)nmb1986Nessuna valutazione finora
- Radiology Search PatternsDocumento19 pagineRadiology Search Patternsnmb19860% (1)
- SOAP Note TemplateDocumento1 paginaSOAP Note Templatenmb1986Nessuna valutazione finora
- Review of SystemsDocumento1 paginaReview of Systemsnmb1986Nessuna valutazione finora
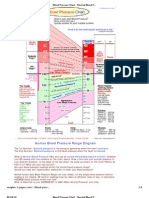
- Blood Pressure ChartDocumento4 pagineBlood Pressure ChartPixelateNessuna valutazione finora
- Transoral Laser MicrosurgeryDocumento4 pagineTransoral Laser MicrosurgeryanniebuhrNessuna valutazione finora
- Mortal Oscillatory Rates - Kook ScienceDocumento20 pagineMortal Oscillatory Rates - Kook ScienceCarl MacCordNessuna valutazione finora
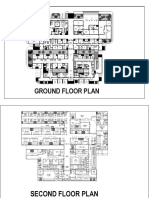
- Sample Plan HospitalDocumento3 pagineSample Plan HospitalMarkNova100% (1)
- IAP Guidelines For FeverDocumento7 pagineIAP Guidelines For FeverVivekanand ChandrakumarNessuna valutazione finora
- BONE Level 2-BDocumento60 pagineBONE Level 2-Bjefri banjarnahorNessuna valutazione finora
- Prioritization Past Medical History of PTB As A Health ThreatDocumento2 paginePrioritization Past Medical History of PTB As A Health ThreatPatrick FormosoNessuna valutazione finora
- Reading Comprehension 4-DikonversiDocumento2 pagineReading Comprehension 4-DikonversiJenifer DoloksaribuNessuna valutazione finora
- 2021 SAISD Mask Mandate-LetterheadDocumento2 pagine2021 SAISD Mask Mandate-LetterheadDavid IbanezNessuna valutazione finora
- Zinc and Copper Levels in Preeclampsia: A Study From Coastal South IndiaDocumento4 pagineZinc and Copper Levels in Preeclampsia: A Study From Coastal South IndiaIriawan Indra PutraNessuna valutazione finora
- 155 PenyakitDocumento112 pagine155 Penyakitpuskesmas kedungdoroNessuna valutazione finora
- HMOLEDocumento12 pagineHMOLEHermie Joy MaglaquiNessuna valutazione finora
- Faktor-Faktor Yang Berhubungan Dengan Terjadinya PreeklampsiaDocumento13 pagineFaktor-Faktor Yang Berhubungan Dengan Terjadinya PreeklampsiaSetiaty PandiaNessuna valutazione finora
- Shampoo in BedDocumento19 pagineShampoo in BedNorman Batalla Juruena, DHCM, PhD, RN92% (13)
- Day2.2 - Lionberger - GDUFA Regulatory ScienceDocumento37 pagineDay2.2 - Lionberger - GDUFA Regulatory ScienceMarkbot1999Nessuna valutazione finora
- Media Children Indpendent Study-4-2Documento21 pagineMedia Children Indpendent Study-4-2api-610458976Nessuna valutazione finora
- Primary Survey & Secondary Survey: Presentor: Shellazianne Anak Ringam Date: 20 November 2015Documento27 paginePrimary Survey & Secondary Survey: Presentor: Shellazianne Anak Ringam Date: 20 November 2015Keluang Man WinchesterNessuna valutazione finora
- Application of Hot Water BagDocumento9 pagineApplication of Hot Water BagDoj Deej Mendoza GambleNessuna valutazione finora
- A SphygmomanometerDocumento3 pagineA Sphygmomanometerdeepesh288Nessuna valutazione finora
- Dengue Hemorrhagic FeverDocumento12 pagineDengue Hemorrhagic FeverzeeNessuna valutazione finora
- Oral Allylestrenol A Pregnancy-Supporting ProgestogenDocumento7 pagineOral Allylestrenol A Pregnancy-Supporting Progestogenjefri efendiNessuna valutazione finora
- Value of A Community-Based Medication ManagementDocumento12 pagineValue of A Community-Based Medication ManagementGetrudeNessuna valutazione finora
- Applicationparent Consent Health FormDocumento5 pagineApplicationparent Consent Health FormBABYLYN TUMBAGANessuna valutazione finora
- Accreditation Of: Health Care SystemDocumento44 pagineAccreditation Of: Health Care SystemFedelyn Mae AcaylarNessuna valutazione finora
- MastoiditisDocumento3 pagineMastoiditisPrincess GyasiNessuna valutazione finora
- Delayed Growth and Development Assessment N.Diagnosis Inference Planning Intervention Rationale EvaluationDocumento2 pagineDelayed Growth and Development Assessment N.Diagnosis Inference Planning Intervention Rationale Evaluationkreny10Nessuna valutazione finora
- Mass General Cover LetterDocumento1 paginaMass General Cover Letterapi-404285262Nessuna valutazione finora
- Osce Book 3rdDocumento39 pagineOsce Book 3rdأحمد الكندي100% (1)
- Integrated Therapeutics IiiDocumento16 pagineIntegrated Therapeutics IiiSalahadinNessuna valutazione finora
- Multiple Chemical Sensitivities - Addendum To Biologic Markers in ImmunotoxicologyDocumento207 pagineMultiple Chemical Sensitivities - Addendum To Biologic Markers in ImmunotoxicologyCarlos RodriguezNessuna valutazione finora
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Da EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Valutazione: 3 su 5 stelle3/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDa EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDValutazione: 5 su 5 stelle5/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDa EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityValutazione: 4 su 5 stelle4/5 (29)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDa EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionValutazione: 4 su 5 stelle4/5 (404)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDa EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNessuna valutazione finora
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDa EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedValutazione: 5 su 5 stelle5/5 (81)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDa EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeValutazione: 2 su 5 stelle2/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDa EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessValutazione: 4.5 su 5 stelle4.5/5 (328)
- The Obesity Code: Unlocking the Secrets of Weight LossDa EverandThe Obesity Code: Unlocking the Secrets of Weight LossValutazione: 4 su 5 stelle4/5 (6)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDa EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDa EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisValutazione: 4.5 su 5 stelle4.5/5 (42)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDa EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsValutazione: 4 su 5 stelle4/5 (4)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDa EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsValutazione: 5 su 5 stelle5/5 (1)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDa EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeValutazione: 4.5 su 5 stelle4.5/5 (253)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Da EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Valutazione: 4.5 su 5 stelle4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDa EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityValutazione: 4 su 5 stelle4/5 (5)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDa EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisValutazione: 4 su 5 stelle4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDa EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryValutazione: 4 su 5 stelle4/5 (45)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDa EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsValutazione: 4.5 su 5 stelle4.5/5 (170)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedDa EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedValutazione: 4 su 5 stelle4/5 (61)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesDa EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesValutazione: 4.5 su 5 stelle4.5/5 (1412)
- How to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingDa EverandHow to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingValutazione: 1 su 5 stelle1/5 (1)
- The Marshmallow Test: Mastering Self-ControlDa EverandThe Marshmallow Test: Mastering Self-ControlValutazione: 4.5 su 5 stelle4.5/5 (59)