Potrebbero piacerti anche
- Medication AdministrationDocumento15 pagineMedication AdministrationbasheNessuna valutazione finora
- Basic Pharmacology HandoutsDocumento16 pagineBasic Pharmacology HandoutsRS BuenavistaNessuna valutazione finora
- Administering Oral MedicationDocumento25 pagineAdministering Oral MedicationAngelo P. VeluzNessuna valutazione finora
- Sost - Funda - Medication AdministrationDocumento8 pagineSost - Funda - Medication AdministrationKYLE SABAYNessuna valutazione finora
- Medication AdministrationDocumento26 pagineMedication AdministrationTuTit100% (2)
- FUNDA Drug Computation AcenaDocumento104 pagineFUNDA Drug Computation AcenaLawrence HanNessuna valutazione finora
- Medication Calculation - Docx..... BDocumento14 pagineMedication Calculation - Docx..... BKaren Ruste Villaluna-AbulenciaNessuna valutazione finora
- Principles of Medication AdministrationDocumento13 paginePrinciples of Medication Administrationloujille89% (9)
- Nclex PharmaDocumento22 pagineNclex Pharmakennedy14344Nessuna valutazione finora
- Drug StudyDocumento7 pagineDrug StudyGladys NacionNessuna valutazione finora
- I Am Sharing 'ATIpharmacologyStudyGuideREVISEDPDF (1) .PDF Version 1' With YouDocumento22 pagineI Am Sharing 'ATIpharmacologyStudyGuideREVISEDPDF (1) .PDF Version 1' With YouGina CatalanoNessuna valutazione finora
- Administration Od DrugsDocumento28 pagineAdministration Od Drugsavenger 2Nessuna valutazione finora
- Principles of Medication AdministrationDocumento22 paginePrinciples of Medication AdministrationTina TalmadgeNessuna valutazione finora
- Oral MedicationsDocumento59 pagineOral MedicationsRaquel MonsalveNessuna valutazione finora
- Pharma LectureDocumento153 paginePharma LectureMike OngNessuna valutazione finora
- Routes of Drug Students)Documento5 pagineRoutes of Drug Students)yabaeve100% (1)
- Administration of Medication (For PHO)Documento56 pagineAdministration of Medication (For PHO)Wondimu EliasNessuna valutazione finora
- Administration and Calculation of Drugs MohDocumento11 pagineAdministration and Calculation of Drugs MohLhen-Vincelyn LeysonNessuna valutazione finora
- Clinical ToxicologyDocumento19 pagineClinical ToxicologyFarina FaraziNessuna valutazione finora
- Nursing Care of The Child Undergoing Medication AdministrationDocumento4 pagineNursing Care of The Child Undergoing Medication Administrationscan1993Nessuna valutazione finora
- Medication AdministrationDocumento82 pagineMedication Administrationbien100% (3)
- Nursing Short Note2Documento35 pagineNursing Short Note2Issac Yasir100% (1)
- Medication AdministrationDocumento100 pagineMedication AdministrationMJ Jomoc ArejolaNessuna valutazione finora
- Phases of Drug DevelopmentDocumento14 paginePhases of Drug DevelopmentMabesNessuna valutazione finora
- Intramuscular InjectionDocumento6 pagineIntramuscular Injectionkiran mahalNessuna valutazione finora
- Medication AdministrationDocumento34 pagineMedication AdministrationSarie Levita100% (2)
- Activity 2 Updated MurilloDocumento22 pagineActivity 2 Updated MurilloAraw GabiNessuna valutazione finora
- Medications Medication: ObjectiveDocumento10 pagineMedications Medication: ObjectiveViolett CatalanNessuna valutazione finora
- Drug Study DMDocumento5 pagineDrug Study DMKimsha ConcepcionNessuna valutazione finora
- Pharmacology NotesDocumento22 paginePharmacology NotesflixiexpressNessuna valutazione finora
- Administrati0n of DrugsDocumento29 pagineAdministrati0n of DrugsJainaba KandehNessuna valutazione finora
- 7 MedicationsDocumento83 pagine7 MedicationsTuTitNessuna valutazione finora
- Pharma Intro and of Drug AdministrationDocumento53 paginePharma Intro and of Drug AdministrationEbiNessuna valutazione finora
- Giving of Medication 12 RightsDocumento41 pagineGiving of Medication 12 RightsLeslie PaguioNessuna valutazione finora
- Drug Study: PART 1: To Be Completed Prior To Clinical ExperienceDocumento5 pagineDrug Study: PART 1: To Be Completed Prior To Clinical ExperienceFrozanSNessuna valutazione finora
- Compilation of QuizzesDocumento10 pagineCompilation of QuizzesElesis samaNessuna valutazione finora
- Medications (Reference: Kozier 8 Edition) : - Written Direction For Preparation & Administration of A DrugDocumento7 pagineMedications (Reference: Kozier 8 Edition) : - Written Direction For Preparation & Administration of A DrugMabesNessuna valutazione finora
- Pharmacology Kechn Notes 2 1Documento85 paginePharmacology Kechn Notes 2 1mbaidavidmutuku1Nessuna valutazione finora
- MedicationsDocumento23 pagineMedicationsYou know whoNessuna valutazione finora
- Pharmacol Finals ReviewerDocumento29 paginePharmacol Finals Reviewerzyyw.abello.uiNessuna valutazione finora
- Medication AdministrationDocumento61 pagineMedication AdministrationdariosumandeNessuna valutazione finora
- Preparing and Administering Oral Medications Basic Concept: Purpose: Assess ForDocumento20 paginePreparing and Administering Oral Medications Basic Concept: Purpose: Assess ForTikTok Trendz100% (1)
- Pharma NotesDocumento5 paginePharma NotesyoojeongredNessuna valutazione finora
- Medication AdministrationDocumento70 pagineMedication Administrationadni_wgNessuna valutazione finora
- Medication AdministrationDocumento88 pagineMedication AdministrationKBD100% (1)
- HESI ReviewerDocumento10 pagineHESI ReviewerAnonymous XhAUv9lp8100% (2)
- Bab IDocumento30 pagineBab Inurliana sariNessuna valutazione finora
- NLN Pharmacology Study GuideDocumento65 pagineNLN Pharmacology Study GuideLauraysha McMillanNessuna valutazione finora
- Review-Guide-in-Pharmacology-Prelim-Exam 2Documento7 pagineReview-Guide-in-Pharmacology-Prelim-Exam 2Marie Allen MadriagaNessuna valutazione finora
- Medication AdmnistrationDocumento34 pagineMedication AdmnistrationAmit MartinNessuna valutazione finora
- Activity No. 2 - DalumpinesDocumento10 pagineActivity No. 2 - DalumpinesJamie Leanne DalumpinesNessuna valutazione finora
- Administering Oral Medications: Melendez, Anna Carmela PDocumento19 pagineAdministering Oral Medications: Melendez, Anna Carmela PAnna Carmela P. MelendezNessuna valutazione finora
- Computation ExercisesDocumento4 pagineComputation Exercisesmysoftware01Nessuna valutazione finora
- 10 RsDocumento5 pagine10 RsNatalie DulawanNessuna valutazione finora
- ManualDocumento13 pagineManualJenelle BernasorNessuna valutazione finora
- Checklist - Medication AdministrationsDocumento37 pagineChecklist - Medication AdministrationsNichola Tappin100% (1)
- HW1 PharmacologyDocumento3 pagineHW1 PharmacologyMICHAEL GABRIEL JIMENEZNessuna valutazione finora
- NCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!Da EverandNCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!Valutazione: 5 su 5 stelle5/5 (4)
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesDa EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesValutazione: 4 su 5 stelle4/5 (2)
- First AidDocumento2 pagineFirst AidDominic ReambonanzaNessuna valutazione finora
- E. A. D. A.: Gastrointestinal SystemDocumento9 pagineE. A. D. A.: Gastrointestinal SystemDominic ReambonanzaNessuna valutazione finora
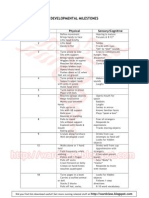
- Developmental MilestonesDocumento2 pagineDevelopmental MilestoneskatyerfeloNessuna valutazione finora
- Normal Values For Common Lab TestsDocumento1 paginaNormal Values For Common Lab Testswyndz100% (6)
- Pharma For StudentsDocumento23 paginePharma For StudentsDominic Reambonanza0% (1)
- PethidineDocumento9 paginePethidineAnonymous VZtcCECtNessuna valutazione finora
- Pocket AnesthesiaDocumento350 paginePocket AnesthesiaBayu Prabowo86% (14)
- Unlock OBGuidelinesPainManagement4Documento30 pagineUnlock OBGuidelinesPainManagement4herry2swNessuna valutazione finora
- Opioid Analgesics - A 2018 Update: SA Pharmaceutical Journal January 2018Documento8 pagineOpioid Analgesics - A 2018 Update: SA Pharmaceutical Journal January 2018Prudhvi Sai NidadavoluNessuna valutazione finora
- Veterinary Pharmacology and Toxicology MCQsDocumento18 pagineVeterinary Pharmacology and Toxicology MCQsSunil97% (63)
- ZOMORPH Capsules 10mgDocumento6 pagineZOMORPH Capsules 10mgFlorexan Malanday PasonNessuna valutazione finora
- BPG Assessment of PainDocumento147 pagineBPG Assessment of PainFarah ShamsudinNessuna valutazione finora
- Organic Medicinal and Pharmaceutical Chemistry AUDocumento109 pagineOrganic Medicinal and Pharmaceutical Chemistry AUAshley DayagNessuna valutazione finora
- Pharmacology OpioidDocumento58 paginePharmacology OpioidCitra Wulandari SofyanNessuna valutazione finora
- The Control of PainDocumento17 pagineThe Control of PainalifafnanNessuna valutazione finora
- Reporting On IV AnestheticsDocumento88 pagineReporting On IV AnestheticsPaul Rizel LedesmaNessuna valutazione finora
- Preanesthetic Medication JasminaDocumento44 paginePreanesthetic Medication Jasminaanjali sNessuna valutazione finora
- Post Anesthesia Care (PACU) GuidelinesDocumento9 paginePost Anesthesia Care (PACU) GuidelinesRaluca LNessuna valutazione finora
- Resource Unit On Common Drugs (LRDR Rotation)Documento37 pagineResource Unit On Common Drugs (LRDR Rotation)kiamoiNessuna valutazione finora
- Fundamentals of Pharmacology 8th Edition Bullock Test BankDocumento9 pagineFundamentals of Pharmacology 8th Edition Bullock Test Bankdorissamuelqpnrrz100% (27)
- Anzca MCQ Saqs Viva Question Bank Pharmacology Including StatisticsDocumento62 pagineAnzca MCQ Saqs Viva Question Bank Pharmacology Including Statisticsالعراقي الصامدNessuna valutazione finora
- Ans KeyDocumento36 pagineAns KeyMarius Clifford BilledoNessuna valutazione finora
- Opioids AutacoidsDocumento22 pagineOpioids AutacoidsSiddharth Anand80% (5)
- List of Narciotic DrugsDocumento8 pagineList of Narciotic DrugsNAVNEET BAGGANessuna valutazione finora
- 5s 4 Draft Opioid AnalgesicsDocumento4 pagine5s 4 Draft Opioid AnalgesicsKim RamosNessuna valutazione finora
- Opoid AnalgesicsDocumento48 pagineOpoid AnalgesicsPratik KhanalNessuna valutazione finora
- Nursing Care Plan UlcerDocumento2 pagineNursing Care Plan Ulcerxrampley2100% (2)
- Cdi 7 - Semifinal ModuleDocumento23 pagineCdi 7 - Semifinal ModuleMary Anne Leal100% (1)
- Central Nervous System MedicationsDocumento12 pagineCentral Nervous System MedicationsMARY JEANINA ALBANessuna valutazione finora
- An Approach To Drug Induced Delirium in The Elderly BMJDocumento7 pagineAn Approach To Drug Induced Delirium in The Elderly BMJLeonela Ramirez Almanza y Lina Maria Ossa HerreraNessuna valutazione finora
- Summativeassessment 3Documento11 pagineSummativeassessment 3api-522946517Nessuna valutazione finora
- Maternal Risk Factors That Should Prompt Anesthesia ConsultationDocumento5 pagineMaternal Risk Factors That Should Prompt Anesthesia ConsultationIsnihaya YusophNessuna valutazione finora
- 5 2TramadolCritReviewDocumento30 pagine5 2TramadolCritReviewyunicaNessuna valutazione finora
- Obsandgyne Tables 200pagesDocumento221 pagineObsandgyne Tables 200pagesRashed ShatnawiNessuna valutazione finora
- Clinical Pharmacokinetics and Pharmacodynamics of Opioid Analgesics in Infants and ChildrenDocumento20 pagineClinical Pharmacokinetics and Pharmacodynamics of Opioid Analgesics in Infants and ChildrenmaryNessuna valutazione finora