Potrebbero piacerti anche
- 13ffd1fa Eda0 4eb8 Bb3a 7802feec40daDocumento40 pagine13ffd1fa Eda0 4eb8 Bb3a 7802feec40daapi-26938624Nessuna valutazione finora
- B0dfbaf2 Beed 4ca7 99fb Ff3588d75dc0Documento3 pagineB0dfbaf2 Beed 4ca7 99fb Ff3588d75dc0api-26938624Nessuna valutazione finora
- c1fd6bbd Ff7a 480d A20e C93bd3a3cedfDocumento35 paginec1fd6bbd Ff7a 480d A20e C93bd3a3cedfapi-26938624Nessuna valutazione finora
- Nervous System IDocumento4 pagineNervous System Iapi-26938624Nessuna valutazione finora
- Lecture 50 April 20th-DiabetesDocumento2 pagineLecture 50 April 20th-Diabetesapi-26938624Nessuna valutazione finora
- Diabetes Mellitus and HypoglycemiaDocumento4 pagineDiabetes Mellitus and Hypoglycemiaapi-26938624Nessuna valutazione finora
- Endocrine System IVDocumento3 pagineEndocrine System IVapi-26938624Nessuna valutazione finora
- Nervous System IIDocumento2 pagineNervous System IIapi-26938624Nessuna valutazione finora
- Endocrine System IIIDocumento3 pagineEndocrine System IIIapi-26938624Nessuna valutazione finora
- Endocrine System IDocumento2 pagineEndocrine System Iapi-26938624Nessuna valutazione finora
- Endorcine System IIDocumento4 pagineEndorcine System IIapi-26938624Nessuna valutazione finora
- Lecture 47 April 13th-EndocrineDocumento1 paginaLecture 47 April 13th-Endocrineapi-26938624Nessuna valutazione finora
- Lecture 42 March 23rd-NervousDocumento2 pagineLecture 42 March 23rd-Nervousapi-26938624Nessuna valutazione finora
- Lecture 48 April 17th-Endocrine (Extra Class)Documento4 pagineLecture 48 April 17th-Endocrine (Extra Class)api-26938624Nessuna valutazione finora
- Lecture 46 April 11th-EndocrineDocumento3 pagineLecture 46 April 11th-Endocrineapi-26938624Nessuna valutazione finora
- Lecture 36 February 28th-Male Genetalia and ReproductionDocumento3 pagineLecture 36 February 28th-Male Genetalia and Reproductionapi-26938624Nessuna valutazione finora
- Lecture 49 April 18th-DiabetesDocumento3 pagineLecture 49 April 18th-Diabetesapi-26938624Nessuna valutazione finora
- Lecture 44 March 30th - NO NOTESDocumento1 paginaLecture 44 March 30th - NO NOTESapi-26938624Nessuna valutazione finora
- Lecture 39 March 9th-MSKDocumento3 pagineLecture 39 March 9th-MSKapi-26938624Nessuna valutazione finora
- Lecture 43 March 28th-NervousDocumento3 pagineLecture 43 March 28th-Nervousapi-26938624Nessuna valutazione finora
- Conditions of The Musculoskeleltal SystemDocumento4 pagineConditions of The Musculoskeleltal Systemapi-26938624Nessuna valutazione finora
- Lecture 45 April 4th-EndocrineDocumento2 pagineLecture 45 April 4th-Endocrineapi-26938624Nessuna valutazione finora
- OP & OA ChartDocumento3 pagineOP & OA Chartapi-26938624100% (1)
- Lecture 37 March 2nd-RenalDocumento2 pagineLecture 37 March 2nd-Renalapi-26938624Nessuna valutazione finora
- Lecture 41 March 16th-NervousDocumento2 pagineLecture 41 March 16th-Nervousapi-26938624Nessuna valutazione finora
- Lecture 35 February 16th-Male Genetalia and ReproductionDocumento3 pagineLecture 35 February 16th-Male Genetalia and Reproductionapi-26938624Nessuna valutazione finora
- Lecture 40 March 14th-MSKDocumento5 pagineLecture 40 March 14th-MSKapi-26938624Nessuna valutazione finora
- DDX - Gastrointestinal Disorders ChartDocumento21 pagineDDX - Gastrointestinal Disorders Chartapi-26938624100% (2)
- Extra DDX NotesDocumento1 paginaExtra DDX Notesapi-26938624Nessuna valutazione finora
- Lecture 33 February 7th-Breast and AxillaDocumento4 pagineLecture 33 February 7th-Breast and Axillaapi-26938624Nessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Comprehensive Exam 1A: Cgfns BootcampDocumento169 pagineComprehensive Exam 1A: Cgfns BootcampmonmonNessuna valutazione finora
- Pituitary Agents PharmaDocumento42 paginePituitary Agents PharmaJayson Tom Briva CapazNessuna valutazione finora
- Study Guide PathoPhysiology UCLA N 230 ADocumento27 pagineStudy Guide PathoPhysiology UCLA N 230 ATracy Pope100% (1)
- Malaysia Paediatric Protocol 3rd EditionDocumento609 pagineMalaysia Paediatric Protocol 3rd EditionSofea Mustaffa100% (7)
- Principles of Fluid Therapy On The Basis ofDocumento29 paginePrinciples of Fluid Therapy On The Basis ofhendrytzNessuna valutazione finora
- Metabolic EncephalopathyDocumento26 pagineMetabolic Encephalopathywirdahaja100% (3)
- Module NCM112 FluidsElectrolytes 2Documento58 pagineModule NCM112 FluidsElectrolytes 2bevzie datuNessuna valutazione finora
- CCRN Review Course 2015Documento81 pagineCCRN Review Course 2015Michelle LindsayNessuna valutazione finora
- Cyclophosphamide Monograph 1june2013 FormattedDocumento12 pagineCyclophosphamide Monograph 1june2013 Formattedpricilia ardianiNessuna valutazione finora
- (1479683X - European Journal of Endocrinology) The Syndrome of Inappropriate Antidiuretic Hormone - Current and Future Management OptionsDocumento6 pagine(1479683X - European Journal of Endocrinology) The Syndrome of Inappropriate Antidiuretic Hormone - Current and Future Management OptionsYulius DonyNessuna valutazione finora
- Ascites in Adults With Cirrhosis - Initial Therapy PDFDocumento28 pagineAscites in Adults With Cirrhosis - Initial Therapy PDFAhraxazel Galicia ReynaNessuna valutazione finora
- Journal Pre-Proof: American Journal of Kidney DiseasesDocumento27 pagineJournal Pre-Proof: American Journal of Kidney DiseasesGabriel Felipe CGNessuna valutazione finora
- Intelligence Is Like A River: The Deeper It Is, The Less Noise It Makes.Documento88 pagineIntelligence Is Like A River: The Deeper It Is, The Less Noise It Makes.reccelle_pre295747Nessuna valutazione finora
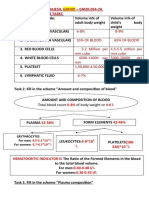
- Name - Soni Ritika Rajesh, Group - GM20-054-2A Physiology Week 03 TasksDocumento10 pagineName - Soni Ritika Rajesh, Group - GM20-054-2A Physiology Week 03 TasksRitika SoniNessuna valutazione finora
- CarbamazepineDocumento41 pagineCarbamazepineHenry SugihartoNessuna valutazione finora
- Me Pediatrics Ntruhs Previous Question Papers Chapter WiseDocumento9 pagineMe Pediatrics Ntruhs Previous Question Papers Chapter WiseNarendra AnnaladasuNessuna valutazione finora
- Guideline On Pediatric Renal - by DR Damte-3Documento172 pagineGuideline On Pediatric Renal - by DR Damte-3Lensa H. BerhanuNessuna valutazione finora
- Homeostasis: Fluids and Electrolytes NCLEX Practice Quiz #2Documento7 pagineHomeostasis: Fluids and Electrolytes NCLEX Practice Quiz #2RJ CarmzNessuna valutazione finora
- ccpc15 Neurocritical Care WorkbookDocumento46 pagineccpc15 Neurocritical Care WorkbookJeremy HamptonNessuna valutazione finora
- Fluids and ElectrolytesDocumento48 pagineFluids and ElectrolytesChernobyle Tolentino BattadNessuna valutazione finora
- Nephrology & Urology: Archer Online USMLE ReviewsDocumento107 pagineNephrology & Urology: Archer Online USMLE ReviewsBeerappaJanpetNessuna valutazione finora
- Hopkins Medicine Review NephrologyDocumento35 pagineHopkins Medicine Review NephrologyMuhammad Bilal50% (2)
- Pediatrics in Review. Dehydration 2015Documento14 paginePediatrics in Review. Dehydration 2015Jorge Eduardo Espinoza Rios100% (2)
- Nephrology MCQ PDFDocumento7 pagineNephrology MCQ PDFreenarachelgeorge100% (4)
- When "Warteg" Gives Him More: Group 7Documento46 pagineWhen "Warteg" Gives Him More: Group 7Daniel Hans JayaNessuna valutazione finora
- Clinical Chemistry (Electrolytes)Documento27 pagineClinical Chemistry (Electrolytes)2B SALVADOR Jamaica C.Nessuna valutazione finora
- Hypernatremia: S. Faubel and J. Topf 8 HypernatremiaDocumento42 pagineHypernatremia: S. Faubel and J. Topf 8 HypernatremiaJoel Topf100% (2)
- Fluid GuidelinesDocumento8 pagineFluid GuidelinesAya SalahNessuna valutazione finora
- MCQDocumento17 pagineMCQBethelhem BerhanuNessuna valutazione finora
- Exam 2 STUDY GUIDEDocumento121 pagineExam 2 STUDY GUIDEJulie BrandtNessuna valutazione finora