Potrebbero piacerti anche
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- 00005Documento7 pagine00005api-3710948Nessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- 00003Documento7 pagine00003api-3710948Nessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Is Condylar Position A Predictor For Functional Signs of TMJ Hypermobility?Documento7 pagineIs Condylar Position A Predictor For Functional Signs of TMJ Hypermobility?api-3710948Nessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Effect of Reclining and Chin-Tuck Position On The Coordination Between Respiration and SwallowingDocumento7 pagineEffect of Reclining and Chin-Tuck Position On The Coordination Between Respiration and Swallowingapi-3710948Nessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- 00004Documento7 pagine00004api-3710948Nessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- 00007Documento1 pagina00007api-3710948Nessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- 00007Documento7 pagine00007api-3710948Nessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Influence of Food Platform Width of Mandibular Removable Partial Denture On Food Mixing AbilityDocumento6 pagineInfluence of Food Platform Width of Mandibular Removable Partial Denture On Food Mixing Abilityapi-3710948Nessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- 00009Documento3 pagine00009api-3710948Nessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- 00004Documento8 pagine00004api-3710948Nessuna valutazione finora
- 00003Documento5 pagine00003api-3710948Nessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- 00008Documento5 pagine00008api-3710948Nessuna valutazione finora
- 00002Documento7 pagine00002api-3710948100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- 00002Documento9 pagine00002api-3710948Nessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Chewing-Side Determination of Three Food Textures: J.Paphangkorakit, N.Thothongkam &N.SupanontDocumento6 pagineChewing-Side Determination of Three Food Textures: J.Paphangkorakit, N.Thothongkam &N.Supanontapi-3710948Nessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Influence of Age and Dental Status On Elevator andDocumento8 pagineThe Influence of Age and Dental Status On Elevator andFlorin LupuNessuna valutazione finora
- 00006Documento5 pagine00006api-3710948Nessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Hardness of Enamel Exposed To Coca-Cola and Artificial SalivaDocumento5 pagineHardness of Enamel Exposed To Coca-Cola and Artificial Salivaapi-3710948Nessuna valutazione finora
- The Functionally Fixed RestorationDocumento6 pagineThe Functionally Fixed Restorationapi-3710948Nessuna valutazione finora
- The Vibratory Characteristics of Obturators With Different Bulb Height and Form DesignsDocumento9 pagineThe Vibratory Characteristics of Obturators With Different Bulb Height and Form Designsapi-3710948Nessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- 00004Documento9 pagine00004api-3710948Nessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Removable Partial Denture EquationDocumento10 pagineThe Removable Partial Denture Equationapi-3710948100% (1)
- Effect of Palate Covering On Bolus-Propulsion Time and Its Contributory FactorsDocumento9 pagineEffect of Palate Covering On Bolus-Propulsion Time and Its Contributory Factorsapi-3710948Nessuna valutazione finora
- Tech RPDDocumento8 pagineTech RPDapi-3710948Nessuna valutazione finora
- RPD Diagnosis, TX PlanningDocumento10 pagineRPD Diagnosis, TX Planningapi-3710948Nessuna valutazione finora
- Partial Dentures in A Dentate WorldDocumento6 paginePartial Dentures in A Dentate Worldapi-37109480% (1)
- SadigDocumento11 pagineSadigapi-3710948Nessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Section 032 RPD ImpressionsDocumento3 pagineSection 032 RPD Impressionsapi-3710948Nessuna valutazione finora
- Management of Patient's Gag Reflex in Making Alginate ImprDocumento2 pagineManagement of Patient's Gag Reflex in Making Alginate Imprapi-3710948Nessuna valutazione finora
- Nzymes Health Skin ProgramDocumento9 pagineNzymes Health Skin Programkshepard_182786911Nessuna valutazione finora
- Overcoming Arthritis - 5th Revised Edition E-BookDocumento89 pagineOvercoming Arthritis - 5th Revised Edition E-Bookmike davis100% (6)
- Newborn Assessment 2.16Documento16 pagineNewborn Assessment 2.16rrbischofbergerNessuna valutazione finora
- Candida Infection, Integrated Science, 4.3Documento13 pagineCandida Infection, Integrated Science, 4.3Anesia Andrews100% (1)
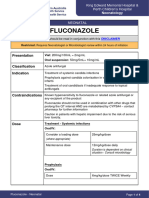
- FluconazoleDocumento4 pagineFluconazoleeucaNessuna valutazione finora
- Pathogenesis:: Candida Albicans in Gram StainingDocumento3 paginePathogenesis:: Candida Albicans in Gram StainingNida RidzuanNessuna valutazione finora
- Mycology NotesDocumento106 pagineMycology NotesRia Alcantara100% (2)
- Generic Name: Classification: Indication:: Candida InfectionsDocumento1 paginaGeneric Name: Classification: Indication:: Candida Infectionscen janber cabrillos0% (1)
- PimafucortDocumento6 paginePimafucortenglish-exactlyNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Neonatal-Perinatal Infections An UpdateDocumento215 pagineNeonatal-Perinatal Infections An Updatebromean.cubitos-0qNessuna valutazione finora
- Antifungal Agents: LipopeptidesDocumento8 pagineAntifungal Agents: LipopeptidesCristian QuitoNessuna valutazione finora
- Pharma Module 3Documento4 paginePharma Module 3Chelsy Sky SacanNessuna valutazione finora
- Fungal Causing DiseasesDocumento9 pagineFungal Causing DiseasesSAMSON, MAXZENE ANICKANessuna valutazione finora
- Current Control Propaganda of Candida Infection Using Dragon FruitDocumento2 pagineCurrent Control Propaganda of Candida Infection Using Dragon FruitEishe Ann GaviolaNessuna valutazione finora
- Candida 1Documento10 pagineCandida 1mufqifitra160491Nessuna valutazione finora
- Cauze BoliDocumento90 pagineCauze BoliSeb SaabNessuna valutazione finora
- Metronidazole AFTinfDocumento8 pagineMetronidazole AFTinfSmartishag BediakoNessuna valutazione finora
- 7.14 Fungi and Fungal DiseaseDocumento25 pagine7.14 Fungi and Fungal DiseaseFN FajrinNessuna valutazione finora
- Guidelines For The Management of Nappy RashDocumento13 pagineGuidelines For The Management of Nappy RashOva PradiptaNessuna valutazione finora
- Antineoplastic MCQDocumento9 pagineAntineoplastic MCQTapas Kumar0% (1)
- Jim LaValle - Atlanta PresentationDocumento222 pagineJim LaValle - Atlanta Presentationtquint23100% (1)
- VaginitisDocumento2 pagineVaginitisFilip JovanovskiNessuna valutazione finora
- Drug Approvals by DCGIDocumento120 pagineDrug Approvals by DCGIVarun HV33% (3)
- Functional Medicine ProtocolDocumento27 pagineFunctional Medicine Protocolmuhjaer100% (5)
- PRESENTED TO: Sir Zafar Iqbal Presented By: Group-EDocumento31 paginePRESENTED TO: Sir Zafar Iqbal Presented By: Group-EAdia MasooraNessuna valutazione finora
- Pharmacology Handout Dr. Ann SpolarichDocumento16 paginePharmacology Handout Dr. Ann SpolarichMina Lotfallah ShenoudaNessuna valutazione finora
- Objectives For Introduction To Medical MycologyDocumento15 pagineObjectives For Introduction To Medical MycologyAlyssa AdamsNessuna valutazione finora
- MycologyDocumento17 pagineMycologyRachana PurohitNessuna valutazione finora
- FUNGAL and PARASITIC INFECTIONSDocumento3 pagineFUNGAL and PARASITIC INFECTIONSKathleen Hazel AndresNessuna valutazione finora