Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Quality-I Is Safety-Ll - The Integration of Two Management Systems - Sasho Andonov (CRC, 2017)Documento205 pagineQuality-I Is Safety-Ll - The Integration of Two Management Systems - Sasho Andonov (CRC, 2017)Tita Eric100% (3)
- How BIM Can Be Utilized To Ensure A Client's Requirements For A Constructions Project Are MetDocumento50 pagineHow BIM Can Be Utilized To Ensure A Client's Requirements For A Constructions Project Are MetHugsNessuna valutazione finora
- SMC System Engineering HandbookDocumento262 pagineSMC System Engineering HandbookThomas BerryNessuna valutazione finora
- Parametric BIM As A Generative Design Tool: Andrzej Zarzycki New Jersey Institute of TechnologyDocumento11 pagineParametric BIM As A Generative Design Tool: Andrzej Zarzycki New Jersey Institute of TechnologyNancy Al-AssafNessuna valutazione finora
- Environmental Modelling & Software: Jan H. KwakkelDocumento12 pagineEnvironmental Modelling & Software: Jan H. Kwakkelelsi narulitaNessuna valutazione finora
- OFMDocumento1 paginaOFMMuhammad AbubakarNessuna valutazione finora
- Knowledge and Practice of Nursing Students Regarding Bioterrorism and Emergency Preparedness: Comparison of The Effects of Simulations and WorkshopDocumento7 pagineKnowledge and Practice of Nursing Students Regarding Bioterrorism and Emergency Preparedness: Comparison of The Effects of Simulations and WorkshopDayana centenoNessuna valutazione finora
- A Steeper Ascent: Growth in The Testing, Inspection and Certification (TIC) IndustryDocumento12 pagineA Steeper Ascent: Growth in The Testing, Inspection and Certification (TIC) IndustryseawoodsNessuna valutazione finora
- Selecting EquipmentDocumento7 pagineSelecting EquipmentZara ShireenNessuna valutazione finora
- Comparing Traffic Simulation Models and the HCMDocumento20 pagineComparing Traffic Simulation Models and the HCMFrancisco GranadosNessuna valutazione finora
- Multiple Intelligences ICT Tools and ApplicationsDocumento19 pagineMultiple Intelligences ICT Tools and Applicationssharpjacqui100% (1)
- III 2015 01 Popovic Kliment Trebuna PekarcikovaDocumento5 pagineIII 2015 01 Popovic Kliment Trebuna PekarcikovajanardhanaNessuna valutazione finora
- Accenture Future of HR Digital Radically DisruptsDocumento16 pagineAccenture Future of HR Digital Radically DisruptsFer ArriagaNessuna valutazione finora
- Modelling Cropping Systems 2002Documento11 pagineModelling Cropping Systems 2002MarcosNessuna valutazione finora
- OptimumTire Product DescriptionDocumento6 pagineOptimumTire Product DescriptionDavid López AlmirallNessuna valutazione finora
- Intelligence, Robotization and Networking for 21st Century ProductionDocumento6 pagineIntelligence, Robotization and Networking for 21st Century ProductionRaghavendra DeshpandeNessuna valutazione finora
- Murtha, J. - Risk Analysis For The Oil IndustryDocumento24 pagineMurtha, J. - Risk Analysis For The Oil IndustryJaime QuirogaNessuna valutazione finora
- Best Practices 05Documento42 pagineBest Practices 05shizatareenNessuna valutazione finora
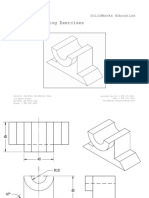
- Detailed Drawing Exercises: Solidworks EducationDocumento51 pagineDetailed Drawing Exercises: Solidworks EducationMajd HusseinNessuna valutazione finora
- Discrete Crack Model For Simulating Rock Comminution Processes With The Discrete Element ModelDocumento9 pagineDiscrete Crack Model For Simulating Rock Comminution Processes With The Discrete Element ModelYesi CeballosNessuna valutazione finora
- Car-Tycoon-Simulator - FINAL Working FileDocumento99 pagineCar-Tycoon-Simulator - FINAL Working FileIrish June TayagNessuna valutazione finora
- Pub - Cooperative Sourcing Simulation Studies and Empiri PDFDocumento483 paginePub - Cooperative Sourcing Simulation Studies and Empiri PDFTanuj BhattacharyyaNessuna valutazione finora
- Sensors: Design and Development of A Novel Invasive Blood Pressure Simulator For Patient's Monitor TestingDocumento19 pagineSensors: Design and Development of A Novel Invasive Blood Pressure Simulator For Patient's Monitor TestingJavier HuarcaNessuna valutazione finora
- Intech Isa Nov - Dec 2012Documento68 pagineIntech Isa Nov - Dec 2012palotito_e100% (1)
- PCD SF 191Documento7 paginePCD SF 191mNessuna valutazione finora
- Automated Car Parking System Using Ros (2) - Read-Only MainDocumento17 pagineAutomated Car Parking System Using Ros (2) - Read-Only Mainvenkatpanuganti58Nessuna valutazione finora
- Digital Age, Current Trends & Ethical Issues in IctDocumento10 pagineDigital Age, Current Trends & Ethical Issues in IctCyril Kaye DolorzoNessuna valutazione finora
- Embedded Coder Getting Started GuideDocumento118 pagineEmbedded Coder Getting Started GuideKjfsa TuNessuna valutazione finora
- CBC Elect Install and Maint NC II 2017Documento63 pagineCBC Elect Install and Maint NC II 2017ralphNessuna valutazione finora
- Organization Study On MRPLDocumento26 pagineOrganization Study On MRPLRavi Baliga K50% (2)