Potrebbero piacerti anche
- Medical CertificateDocumento3 pagineMedical CertificateSñëhå PàlNessuna valutazione finora
- 5976df9ea1fa813 5190126793 PDFDocumento1 pagina5976df9ea1fa813 5190126793 PDFPsycho SoldierNessuna valutazione finora
- Medical Leave CertificateDocumento1 paginaMedical Leave Certificatenetcity143Nessuna valutazione finora
- Medical CertificateDocumento1 paginaMedical CertificateSaiyed IqbalNessuna valutazione finora
- Medical Leave Proforma 20200612132007Documento4 pagineMedical Leave Proforma 20200612132007Dhana LakshmiNessuna valutazione finora
- Certificate of Fitness To Return To Duty: Kalvisigaram-TngtfaDocumento1 paginaCertificate of Fitness To Return To Duty: Kalvisigaram-Tngtfamjcare100% (1)
- Medical Fitness Certificate PDFDocumento1 paginaMedical Fitness Certificate PDFMuhammed FarisNessuna valutazione finora
- Medical Certificate For LeavDocumento1 paginaMedical Certificate For LeavKrishnaswamy RajaNessuna valutazione finora
- Medical Certificate For Leave - Gaz OfficerDocumento1 paginaMedical Certificate For Leave - Gaz OfficerJayakrishna ReddyNessuna valutazione finora
- Section - 3 Medical Fitness CertificateDocumento1 paginaSection - 3 Medical Fitness CertificateireneNessuna valutazione finora
- Medical Leave Proforma 20200612132007Documento4 pagineMedical Leave Proforma 20200612132007Nathiya100% (1)
- Medical Certificate FormatDocumento1 paginaMedical Certificate FormatVikrant MishraNessuna valutazione finora
- Form Ama PDFDocumento1 paginaForm Ama PDFLOVI KRISSADINessuna valutazione finora
- Med Cert StudentDocumento1 paginaMed Cert StudentPriyadharshan EzioNessuna valutazione finora
- Medical Fitness Certificate 1Documento1 paginaMedical Fitness Certificate 1Daryll Dela PazNessuna valutazione finora
- FORM 4 (See Rules 19) Medical Certificate For Non-Gazetted Officers Recommended Leave or Extension of Leave or Commutation of LeaveDocumento1 paginaFORM 4 (See Rules 19) Medical Certificate For Non-Gazetted Officers Recommended Leave or Extension of Leave or Commutation of LeaveSaurabh SingraoreNessuna valutazione finora
- Medical Certificate Form for Govt Servant LeaveDocumento1 paginaMedical Certificate Form for Govt Servant Leaveamit_saxena_10Nessuna valutazione finora
- Tac Appendix 5Documento1 paginaTac Appendix 5Anbaraj Arun100% (2)
- Form - E: (See Rule 9 and 10)Documento1 paginaForm - E: (See Rule 9 and 10)vishalsolsheNessuna valutazione finora
- FORM C - Register of Unpaid AccumulationsDocumento1 paginaFORM C - Register of Unpaid AccumulationsSailaja Subramanyam100% (1)
- Form - E (See Rule 9 and 10) Certificate: (To Be Given by The Medical Officer of Not Below The Rank of District Surgeons)Documento1 paginaForm - E (See Rule 9 and 10) Certificate: (To Be Given by The Medical Officer of Not Below The Rank of District Surgeons)Shantanu Bhardwaj100% (1)
- Certificate of Physical Fitness FormDocumento3 pagineCertificate of Physical Fitness Formraghavbiduru1100% (1)
- Certificat Medical ModeleDocumento1 paginaCertificat Medical ModeleAdèle SchwannerNessuna valutazione finora
- Helmet Removal TechniquesDocumento21 pagineHelmet Removal TechniquesHizam Zulfhi100% (1)
- Medical Leave FormsDocumento2 pagineMedical Leave FormsSudhakar ChollangiNessuna valutazione finora
- Character CertificateDocumento1 paginaCharacter CertificateAzad KhanNessuna valutazione finora
- Form 4 (Medical Certificate For Leave or Extension or Leave)Documento1 paginaForm 4 (Medical Certificate For Leave or Extension or Leave)shekhar.mnnitNessuna valutazione finora
- Physical Fitness CertificateDocumento1 paginaPhysical Fitness CertificateAllu ReddyNessuna valutazione finora
- Freshers Application for InfosysDocumento2 pagineFreshers Application for InfosysveersinglaNessuna valutazione finora
- Pocedure ConsentDocumento2 paginePocedure ConsentJack TedescoNessuna valutazione finora
- Conditional AssignmentDocumento1 paginaConditional AssignmentVarsha ThampiNessuna valutazione finora
- (See Rule 4) The Maternity Benefit Rules, 1961: Form BDocumento1 pagina(See Rule 4) The Maternity Benefit Rules, 1961: Form BAbhishek Mishra100% (1)
- Medical Certificate FormatDocumento1 paginaMedical Certificate FormatrashmarsvNessuna valutazione finora
- Format of Application For PeonDocumento1 paginaFormat of Application For Peonsanjaya behera100% (1)
- Medical leave applicationDocumento3 pagineMedical leave applicationSreeraj B PillaiNessuna valutazione finora
- Medical CertificateDocumento1 paginaMedical CertificateMountsinai CscNessuna valutazione finora
- Emergency CertificateDocumento1 paginaEmergency Certificateapi-3710215Nessuna valutazione finora
- Consent FormDocumento1 paginaConsent FormJohn BestNessuna valutazione finora
- Employee Drug Testing Consent FormDocumento1 paginaEmployee Drug Testing Consent FormRocketLawyer0% (1)
- Medical Fitness Kerala PSCDocumento1 paginaMedical Fitness Kerala PSCDhanush PvNessuna valutazione finora
- Employment Application 0Documento5 pagineEmployment Application 0Charles ValenzuelaNessuna valutazione finora
- No 55+the+Secrets+of+Organic+SulphurDocumento2 pagineNo 55+the+Secrets+of+Organic+Sulphurwterry2Nessuna valutazione finora
- Life Certificate - ServiceDocumento1 paginaLife Certificate - ServiceSuraj Chavan100% (1)
- Renew Your Physiotherapy LicenseDocumento3 pagineRenew Your Physiotherapy LicenseShrikant SantNessuna valutazione finora
- Certificate of Health: Form No. 42Documento1 paginaCertificate of Health: Form No. 42AshwathyNessuna valutazione finora
- Physical fitness certificateDocumento1 paginaPhysical fitness certificateEluri Mahesh NaniNessuna valutazione finora
- Medical Certificate CorrecetdDocumento1 paginaMedical Certificate CorrecetdSerigneTackoNgomNessuna valutazione finora
- VAS Physical Fitness Certificate FormatDocumento1 paginaVAS Physical Fitness Certificate FormatpmarkandayNessuna valutazione finora
- Medical Certificate Form PDFDocumento1 paginaMedical Certificate Form PDFbusiness.aadityayadavNessuna valutazione finora
- Medical Leave CertificatesDocumento4 pagineMedical Leave CertificatesDhana LakshmiNessuna valutazione finora
- 5976df9ea1fa813 5190126793 PDFDocumento1 pagina5976df9ea1fa813 5190126793 PDFGautamNessuna valutazione finora
- Medical Certificate and FitnessDocumento1 paginaMedical Certificate and FitnessmanuelmathewsNessuna valutazione finora
- Sicknessandfitnesscertificates PDFDocumento6 pagineSicknessandfitnesscertificates PDFniraj_sdNessuna valutazione finora
- B CertDocumento2 pagineB Certm.arunNessuna valutazione finora
- Medical Certificate FormatDocumento1 paginaMedical Certificate FormatKausy VaradkarNessuna valutazione finora
- Medical CertificateDocumento1 paginaMedical CertificateNakul KulkarniNessuna valutazione finora
- Certificate of Physical Fitness by A Single Medical OfficerDocumento1 paginaCertificate of Physical Fitness by A Single Medical OfficerBalu Ramachandran68% (28)
- Advance Medical DirectiveDocumento2 pagineAdvance Medical DirectiveAmisha PrakashNessuna valutazione finora
- Medical Fitness CertificateDocumento1 paginaMedical Fitness CertificateireneNessuna valutazione finora
- Medical Essential Certificate-ADocumento2 pagineMedical Essential Certificate-AShahed HusaainNessuna valutazione finora
- Reinforced EarthDocumento16 pagineReinforced EarthseshuNessuna valutazione finora
- V.tank DetailDocumento1 paginaV.tank DetailseshuNessuna valutazione finora
- Flat Slab DesignDocumento76 pagineFlat Slab Designyunuswsa97% (36)
- Piers GFDocumento4 paginePiers GFseshuNessuna valutazione finora
- Nit SezDocumento5 pagineNit SezseshuNessuna valutazione finora
- Problems On Centre of Pressure PDFDocumento5 pagineProblems On Centre of Pressure PDFseshu0% (1)
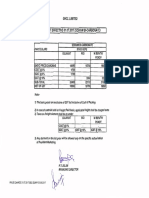
- Effective From ArbonateDocumento1 paginaEffective From ArbonateseshuNessuna valutazione finora
- Grid/ Waffle Slab: Compiled By, Submitted ToDocumento21 pagineGrid/ Waffle Slab: Compiled By, Submitted ToseshuNessuna valutazione finora
- Electronic Total StationDocumento2 pagineElectronic Total StationseshuNessuna valutazione finora
- Capped Pile Type Piers - Portions of H-Piling Completely Rusted ThroughDocumento1 paginaCapped Pile Type Piers - Portions of H-Piling Completely Rusted ThroughseshuNessuna valutazione finora
- Survey and Geotechnical Investigation Works For The Preparation of Detailed Project Report of Proposed Gargai DamDocumento1 paginaSurvey and Geotechnical Investigation Works For The Preparation of Detailed Project Report of Proposed Gargai DamseshuNessuna valutazione finora
- NIT Geophysical Narlapur DindiDocumento1 paginaNIT Geophysical Narlapur DindiseshuNessuna valutazione finora
- EstimationsDocumento34 pagineEstimationsShabbeer009Nessuna valutazione finora
- WAPCOS Corrigendum Extends Deadline for Odisha Hydropower Project TenderDocumento1 paginaWAPCOS Corrigendum Extends Deadline for Odisha Hydropower Project TenderseshuNessuna valutazione finora
- Ziao Syey MehDocumento15 pagineZiao Syey MehseshuNessuna valutazione finora
- Map VLGDocumento3 pagineMap VLGseshuNessuna valutazione finora
- Government of Andhra Pradesh Government of Andhra Pradesh: Subject SubjectDocumento21 pagineGovernment of Andhra Pradesh Government of Andhra Pradesh: Subject SubjectseshuNessuna valutazione finora
- The Hon'Ble Sri Justice A.V.Sesha Sai WRIT PETITION No.8596 of 2017 OrderDocumento3 pagineThe Hon'Ble Sri Justice A.V.Sesha Sai WRIT PETITION No.8596 of 2017 OrderseshuNessuna valutazione finora
- 23Documento1 pagina23seshuNessuna valutazione finora
- Total LayoutsDocumento1 paginaTotal LayoutsseshuNessuna valutazione finora
- G O RT No 409Documento2 pagineG O RT No 409seshuNessuna valutazione finora
- 2Documento4 pagine2seshuNessuna valutazione finora
- Petro Terminology-Guide PDFDocumento12 paginePetro Terminology-Guide PDFseshuNessuna valutazione finora
- Operational Considerations of Hard Rockaggregate QuarriesDocumento2 pagineOperational Considerations of Hard Rockaggregate QuarriesseshuNessuna valutazione finora
- RCC Design by BC Punmia PDFDocumento924 pagineRCC Design by BC Punmia PDFmishrajayesh17Nessuna valutazione finora
- Updated: March 21, 2017 09:22 (IST) : SakshiDocumento2 pagineUpdated: March 21, 2017 09:22 (IST) : SakshiseshuNessuna valutazione finora
- Blast PatternsDocumento10 pagineBlast Patternsrajasekar21Nessuna valutazione finora
- Tunnelling Methods1 121019223907 Phpapp02Documento34 pagineTunnelling Methods1 121019223907 Phpapp02laurenjiaNessuna valutazione finora
- SoR 2016-17 (PART-I, II, III&IV) 29.11.2016Documento530 pagineSoR 2016-17 (PART-I, II, III&IV) 29.11.2016seshuNessuna valutazione finora