Potrebbero piacerti anche
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!Da EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!Nessuna valutazione finora
- ECG and ArrhythmiasDocumento25 pagineECG and ArrhythmiasRashed ShatnawiNessuna valutazione finora
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsDa EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNessuna valutazione finora
- EKG InterpretationDocumento65 pagineEKG Interpretationpaskariatne probo dewi100% (1)
- Pakya ECG BasicsDocumento5 paginePakya ECG BasicsFrederick CokroNessuna valutazione finora
- EKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationDa EverandEKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationValutazione: 3 su 5 stelle3/5 (1)
- ECG InterpretationDocumento40 pagineECG InterpretationMuhammad BadrushshalihNessuna valutazione finora
- ECG TutorialDocumento40 pagineECG TutorialAnonymous HAbhRTs2TfNessuna valutazione finora
- Simple Guide To Ecg InterpretationDocumento53 pagineSimple Guide To Ecg Interpretationedy suyantoNessuna valutazione finora
- ECG ReadingDocumento11 pagineECG ReadingSuresh Shrestha100% (1)
- Wolff-Parkinson- White-Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandWolff-Parkinson- White-Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Basic Arrhythmia RulesDocumento3 pagineBasic Arrhythmia Rulesgreenflames0997% (30)
- ECG Interpretation - Axis and Conduction AbnormalitiesDocumento9 pagineECG Interpretation - Axis and Conduction Abnormalitiesradha1000100% (1)
- EKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasDa EverandEKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasValutazione: 3 su 5 stelle3/5 (5)
- Reading A EKGDocumento10 pagineReading A EKGMayer Rosenberg100% (15)
- Torsade De Pointes, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandTorsade De Pointes, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Cardiac Rhythms and DysrhythmiasDocumento14 pagineCardiac Rhythms and DysrhythmiasShawn Gaurav Jha100% (1)
- EKG Interpretation: Making EKG/ECG Interpretation Easy!Da EverandEKG Interpretation: Making EKG/ECG Interpretation Easy!Nessuna valutazione finora
- EKG Pocket GuideDocumento2 pagineEKG Pocket GuideFabian Ramirez HincapiéNessuna valutazione finora
- May/No P: Inverted/B/ A Qrs P (Befor e QRS) - 0.12Documento3 pagineMay/No P: Inverted/B/ A Qrs P (Befor e QRS) - 0.12is_aradanas0% (1)
- ECG Mastery Improving Your ECG Interpretation SkillsDocumento23 pagineECG Mastery Improving Your ECG Interpretation SkillsHitesh Deora100% (2)
- ECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!Da EverandECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!Nessuna valutazione finora
- Dysrhythmias ChartDocumento6 pagineDysrhythmias Chartjkrix100% (1)
- Cardiac Tamponade, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandCardiac Tamponade, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Mini Test QUIZDocumento9 pagineMini Test QUIZAbdul RohimNessuna valutazione finora
- Ecg Reading NotesDocumento17 pagineEcg Reading NotesMarian FloresNessuna valutazione finora
- ArrhythmiaDocumento2 pagineArrhythmiaChris Pritchard93% (30)
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsNessuna valutazione finora
- Ecg Cheat Sheet 35Documento2 pagineEcg Cheat Sheet 35jessjaylee80% (5)
- Ekg Strip NotesDocumento13 pagineEkg Strip NotesNick Loizzo100% (2)
- Ecg Essentials 2 PDFDocumento45 pagineEcg Essentials 2 PDFjaikishan marathe 69Nessuna valutazione finora
- Basic EKG For DummiesDocumento133 pagineBasic EKG For Dummieseduardocmoura86% (7)
- Spotlight On Cardiac DrugsDocumento2 pagineSpotlight On Cardiac Drugspauerish100% (2)
- Cardiac DysrhythmiasDocumento3 pagineCardiac DysrhythmiasKatherine Santiago92% (62)
- Ecg Taking and Interpretation.... PowerpointDocumento37 pagineEcg Taking and Interpretation.... PowerpointJara Maris Moreno BudionganNessuna valutazione finora
- EKG Rhythms2 PDFDocumento7 pagineEKG Rhythms2 PDFAya KamajayaNessuna valutazione finora
- ECG StripsDocumento5 pagineECG StripsNursingSchoolNotes100% (1)
- EKG Practice TestDocumento16 pagineEKG Practice TestAbdul Rohim100% (1)
- Advanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineDocumento88 pagineAdvanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineRoroNessuna valutazione finora
- Cardiac MedicationsDocumento9 pagineCardiac Medicationsnovikane100% (1)
- EKG RhythmsDocumento10 pagineEKG RhythmsQueenNessuna valutazione finora
- ACLS PharmacologyDocumento5 pagineACLS PharmacologyKuruva MallikarjunaNessuna valutazione finora
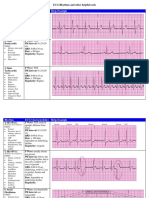
- Rhythm ECG Characteristics Strip Example: ECG Rhythms and Other Helpful ToolsDocumento6 pagineRhythm ECG Characteristics Strip Example: ECG Rhythms and Other Helpful ToolsJohnildy MatiasNessuna valutazione finora
- A Simplified ECG GuideDocumento4 pagineA Simplified ECG Guidejalan_z96% (27)
- EKG Quick Reference ChartDocumento4 pagineEKG Quick Reference ChartMildaNessuna valutazione finora
- Recognizing Normal ECGDocumento50 pagineRecognizing Normal ECGJosiephine Bucalon100% (3)
- EKG ExamplesDocumento9 pagineEKG ExamplesMayer Rosenberg99% (235)
- Acid-Base WorksheetDocumento2 pagineAcid-Base WorksheetMayer Rosenberg100% (18)
- Rhythm Interpretation and Its ManagementDocumento6 pagineRhythm Interpretation and Its Managementjh_ajjNessuna valutazione finora
- Common Cardiac MedicationsDocumento1 paginaCommon Cardiac MedicationsPaige HardekopfNessuna valutazione finora
- Basic ECG and Arrhythmia FINALDocumento16 pagineBasic ECG and Arrhythmia FINALCharlotte James100% (5)
- Pulmonary Leukostasis Mimicking Pulmonary Embolism: Case of The MonthDocumento4 paginePulmonary Leukostasis Mimicking Pulmonary Embolism: Case of The MonthkaremiaNessuna valutazione finora
- Seaweed InvasionsDocumento153 pagineSeaweed InvasionsLeonardo Souza LimaNessuna valutazione finora
- CH 03Documento36 pagineCH 03abdurNessuna valutazione finora
- Group Case Study Obstetrics Group 5 From SMUDocumento84 pagineGroup Case Study Obstetrics Group 5 From SMUJosephine Mae TumanutNessuna valutazione finora
- The Nervous SystemDocumento5 pagineThe Nervous SystemArif QadhafyNessuna valutazione finora
- Nitrogen CycleDocumento10 pagineNitrogen CyclebellaNessuna valutazione finora
- AnswersDocumento91 pagineAnswersAndy Alvarez100% (1)
- Shoku AnafilaktikDocumento16 pagineShoku AnafilaktikindeenikeNessuna valutazione finora
- Summative Test-G8-Quarter-4Documento13 pagineSummative Test-G8-Quarter-4Charmaine CanonoNessuna valutazione finora
- Edexcel GCSE Science Topic B1.1 Classification, Variation and Inheritance Test 13 - 14Documento10 pagineEdexcel GCSE Science Topic B1.1 Classification, Variation and Inheritance Test 13 - 14Paul BurgessNessuna valutazione finora
- Patente Endoesqueleto para Sex Doll SiliconaDocumento12 paginePatente Endoesqueleto para Sex Doll SiliconaGabriel De Jesus100% (1)
- Question PaperDocumento16 pagineQuestion PaperAashi AkterNessuna valutazione finora
- Comprehensive Head To Toe Assessment PDFDocumento22 pagineComprehensive Head To Toe Assessment PDFVanessaMUellerNessuna valutazione finora
- Endocrine Glands RevisedDocumento47 pagineEndocrine Glands RevisedXyress Archer GosinganNessuna valutazione finora
- Antioxidants !! The Great DiscoveryDocumento3 pagineAntioxidants !! The Great DiscoverypatNessuna valutazione finora
- RPD ImpressionDocumento49 pagineRPD ImpressionAmar Bimavarapu0% (1)
- Comparative Anatomy Study of The Respiratory System Between Green Turtle (Chelonia Mydas) and Leatherback Turtle (Dermochelys Coriacea)Documento1 paginaComparative Anatomy Study of The Respiratory System Between Green Turtle (Chelonia Mydas) and Leatherback Turtle (Dermochelys Coriacea)AldinaNessuna valutazione finora
- As Biology With Stafford Unit 3 Workbook Answers PDFDocumento21 pagineAs Biology With Stafford Unit 3 Workbook Answers PDFFatma ZorluNessuna valutazione finora
- Skeletal StructureDocumento58 pagineSkeletal StructureCsd AutoprimNessuna valutazione finora
- The Truth About Lie Detectors Aka Polygraph TestsDocumento4 pagineThe Truth About Lie Detectors Aka Polygraph TestsMălina-Ionela CorlătianuNessuna valutazione finora
- Toltec Body Healing EbookDocumento204 pagineToltec Body Healing EbookDanielle Grace100% (3)
- FA 2014 RenalRespDocumento118 pagineFA 2014 RenalResprvar839Nessuna valutazione finora
- Funda 7Documento19 pagineFunda 7Akia Cayasan BayaNessuna valutazione finora
- ADR Common Drug - Induced Organ DisordersDocumento45 pagineADR Common Drug - Induced Organ Disorders0009439Nessuna valutazione finora
- Hemolytic Uremic SyndromeDocumento1 paginaHemolytic Uremic SyndromeAndrea TeranNessuna valutazione finora
- Practice Test Questions Downloaded From FILIPINO NURSES CENTRALDocumento5 paginePractice Test Questions Downloaded From FILIPINO NURSES CENTRALFilipino Nurses CentralNessuna valutazione finora
- Adult Health Final Study GuideDocumento5 pagineAdult Health Final Study GuideNurseNancy93100% (1)
- Endocrine and Metabolic Disorders PDFDocumento31 pagineEndocrine and Metabolic Disorders PDFAna-Maria50% (2)
- DISACCHARIDES Lecture For 1st Year MBBS Delivered by Dr. Waseem On 01 March 2010Documento29 pagineDISACCHARIDES Lecture For 1st Year MBBS Delivered by Dr. Waseem On 01 March 2010IMDCBiochemNessuna valutazione finora
- Zabrina Joana DDocumento4 pagineZabrina Joana DEmman BalidoNessuna valutazione finora
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Da EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Valutazione: 3 su 5 stelle3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDa EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedValutazione: 4.5 su 5 stelle4.5/5 (82)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDa EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDValutazione: 5 su 5 stelle5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDa EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionValutazione: 4 su 5 stelle4/5 (404)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDa EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityValutazione: 4 su 5 stelle4/5 (32)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDa EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeValutazione: 2 su 5 stelle2/5 (1)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesDa EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesValutazione: 4.5 su 5 stelle4.5/5 (1412)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDa EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNessuna valutazione finora
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDa EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsValutazione: 4 su 5 stelle4/5 (4)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDa EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsValutazione: 5 su 5 stelle5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDa EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisValutazione: 4.5 su 5 stelle4.5/5 (42)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDa EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Obesity Code: Unlocking the Secrets of Weight LossDa EverandThe Obesity Code: Unlocking the Secrets of Weight LossValutazione: 4 su 5 stelle4/5 (6)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDa EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityValutazione: 4.5 su 5 stelle4.5/5 (6)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDa EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisValutazione: 3.5 su 5 stelle3.5/5 (2)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDa EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeValutazione: 4.5 su 5 stelle4.5/5 (254)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Da EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Valutazione: 4.5 su 5 stelle4.5/5 (110)
- To Explain the World: The Discovery of Modern ScienceDa EverandTo Explain the World: The Discovery of Modern ScienceValutazione: 3.5 su 5 stelle3.5/5 (51)