Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- AZUSA Ministry Training Institute Non-Degree ApplicationDocumento9 pagineAZUSA Ministry Training Institute Non-Degree ApplicationAZUSA World Ministries Ministry Training InstituteNessuna valutazione finora
- The Atom: Cornell Doodle NotesDocumento22 pagineThe Atom: Cornell Doodle NotesSalina SalujaNessuna valutazione finora
- Non-Degree Fee ScheduleDocumento1 paginaNon-Degree Fee ScheduleAZUSA World Ministries Ministry Training InstituteNessuna valutazione finora
- AZUSA Members Degree Fee Schedule: Books Not Included (Notes Included)Documento1 paginaAZUSA Members Degree Fee Schedule: Books Not Included (Notes Included)AZUSA World Ministries Ministry Training InstituteNessuna valutazione finora
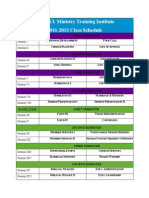
- AZUSA MTI Class Schedule For Blocks 3&4Documento1 paginaAZUSA MTI Class Schedule For Blocks 3&4AZUSA World Ministries Ministry Training InstituteNessuna valutazione finora
- AZUSA World Ministries ABI - Class - SchedDocumento1 paginaAZUSA World Ministries ABI - Class - SchedAZUSA World Ministries Ministry Training InstituteNessuna valutazione finora
- Notes Microwave Engineering Unit 5 PDFDocumento14 pagineNotes Microwave Engineering Unit 5 PDFKujur RebecaNessuna valutazione finora
- Slow LearnerDocumento33 pagineSlow LearnerMuhammad Khairul Nizam100% (1)
- Bilingual First Language Acquisition: January 2008Documento11 pagineBilingual First Language Acquisition: January 2008Katsiaryna HurbikNessuna valutazione finora
- Byzantium Notes CultureDocumento6 pagineByzantium Notes Culturepatrick cairoliNessuna valutazione finora
- Key Professional DispositionsDocumento3 pagineKey Professional DispositionsEmily SneedNessuna valutazione finora
- Self-Assessment Observation and Assessment of Child DevelopmentDocumento3 pagineSelf-Assessment Observation and Assessment of Child Developmentapi-508676940Nessuna valutazione finora
- AwanishTrivedi PastryChefDocumento3 pagineAwanishTrivedi PastryChefChandra MohanNessuna valutazione finora
- CSPL v1.2.0 Install-Eng Memo1Documento3 pagineCSPL v1.2.0 Install-Eng Memo1rammirisNessuna valutazione finora
- Tutorial Week 10 Topic 9Documento14 pagineTutorial Week 10 Topic 9patricia93limNessuna valutazione finora
- Manual Stiga VILLA 92 MDocumento6 pagineManual Stiga VILLA 92 MCzesław WierzchowskiNessuna valutazione finora
- Final Coaching - FundaDocumento3 pagineFinal Coaching - FundaenzoNessuna valutazione finora
- Arquitectura de SoftwareDocumento6 pagineArquitectura de SoftwareDiego Alejandro Muñoz ToroNessuna valutazione finora
- Blast Injury ManagementDocumento16 pagineBlast Injury Managementheart wisdomNessuna valutazione finora
- Aakash ADV Full Tests MERGEDDocumento486 pagineAakash ADV Full Tests MERGEDAnirudh100% (1)
- IRC CodesDocumento23 pagineIRC CodesabhijithavalNessuna valutazione finora
- Big Breakfasts Help Us Burn Double The CaloriesDocumento4 pagineBig Breakfasts Help Us Burn Double The CaloriesBastian IgnacioNessuna valutazione finora
- Discuss The Nature and Extent of Slavery As An Institution in Greco-Roman SocietyDocumento4 pagineDiscuss The Nature and Extent of Slavery As An Institution in Greco-Roman SocietySouravNessuna valutazione finora
- X Ray DiffractionDocumento12 pagineX Ray DiffractionSiddraKhalidNessuna valutazione finora
- Guidelines For Mental Care Onboard Merchant Ships: ContentDocumento12 pagineGuidelines For Mental Care Onboard Merchant Ships: ContentSona NarulaNessuna valutazione finora
- GP150 PDFDocumento125 pagineGP150 PDFBf Ipanema100% (1)
- The BoarderDocumento3 pagineThe BoarderAnonymous iX6KV9LZzoNessuna valutazione finora
- Noise FigureDocumento17 pagineNoise FigureManel CharlesNessuna valutazione finora
- Inorganic Chemistry MatriculationDocumento46 pagineInorganic Chemistry MatriculationShinta Novita Sari100% (1)
- Future Tower Iii, Sharjah: Operation & Maintenance Manual Building Maintenance UnitDocumento107 pagineFuture Tower Iii, Sharjah: Operation & Maintenance Manual Building Maintenance UnitFrancis BautistaNessuna valutazione finora
- Geometri Unsur StrukturDocumento10 pagineGeometri Unsur StrukturNirmaya WulandariNessuna valutazione finora
- Exercises Problem 2 Lesson 4Documento2 pagineExercises Problem 2 Lesson 4Marianne DevillenaNessuna valutazione finora
- Internet BillDocumento2 pagineInternet Billshiva ramNessuna valutazione finora
- Mod6 4Documento10 pagineMod6 4mn3mNessuna valutazione finora
- Chapter 1Documento17 pagineChapter 1Nari KangNessuna valutazione finora