Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Part A-8-Proving Child Survival RatesDocumento7 paginePart A-8-Proving Child Survival RatesdarylNessuna valutazione finora
- Department of Education: Wash in Schools Programs (WINS)Documento5 pagineDepartment of Education: Wash in Schools Programs (WINS)RONALYN ALVAREZNessuna valutazione finora
- Angel Khaille L. Saguban - Final TaskDocumento1 paginaAngel Khaille L. Saguban - Final TaskAngel SagubanNessuna valutazione finora
- Argumentative EssayDocumento8 pagineArgumentative EssayGabriel SarteNessuna valutazione finora
- Food Adulteration and HygieneDocumento30 pagineFood Adulteration and HygieneSandesh Paudel100% (2)
- ADA Cal en DT ADS001150 Rev01Documento1 paginaADA Cal en DT ADS001150 Rev01vijayramaswamyNessuna valutazione finora
- State Magazine, September 2003Documento44 pagineState Magazine, September 2003State MagazineNessuna valutazione finora
- EngDocumento244 pagineEngIntan IntanNessuna valutazione finora
- HEALTH FORM RSCC 1Documento4 pagineHEALTH FORM RSCC 1Garlyn TaycoNessuna valutazione finora
- Microflora PericoronariteDocumento45 pagineMicroflora PericoronariteCeresău MarinaNessuna valutazione finora
- Multiple Choice TestDocumento3 pagineMultiple Choice TestJane Kennith FebrioNessuna valutazione finora
- Cholycystectomy FinalDocumento53 pagineCholycystectomy FinalCharmie GandaNessuna valutazione finora
- GasiDocumento36 pagineGasiAdy Fitra Saragih100% (1)
- Multiple Choice QuestionsDocumento5 pagineMultiple Choice QuestionsDr Sumant Sharma80% (10)
- Adulterants in Food Investigatory ProjectDocumento16 pagineAdulterants in Food Investigatory ProjectNeha Koul0% (1)
- Differential Diagnosis of T2 Hyperintense Brainstem Lesions: Part 2. Diffuse LesionsDocumento15 pagineDifferential Diagnosis of T2 Hyperintense Brainstem Lesions: Part 2. Diffuse LesionsPreetiReddyNessuna valutazione finora
- Introduction To EpidemiologyDocumento87 pagineIntroduction To EpidemiologyMugisha Laurian100% (1)
- Genital MutilationDocumento2 pagineGenital MutilationDanitza Cárdenas LingüisTICs CONessuna valutazione finora
- Adenotonsillar Disease BastaninejadDocumento52 pagineAdenotonsillar Disease BastaninejadArbusa86Nessuna valutazione finora
- Avenue of PenetrationDocumento3 pagineAvenue of Penetrationshyamsunder68100% (1)
- Uxz PDFDocumento16 pagineUxz PDFSaifur RahmanNessuna valutazione finora
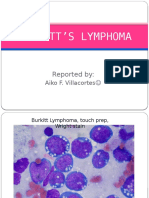
- Burkitt S LymphomaDocumento12 pagineBurkitt S LymphomaAiko VillacortesNessuna valutazione finora
- 559-Skim Milk-115363Documento1 pagina559-Skim Milk-115363Yurina HaryantiNessuna valutazione finora
- Biostatistics and Role in DentistryDocumento90 pagineBiostatistics and Role in DentistryJyoti Sharma100% (1)
- Practical Research 1 Group 54 Qualitative ResearchDocumento2 paginePractical Research 1 Group 54 Qualitative ResearchMadielyn SalomeroNessuna valutazione finora
- Lesson Plan Cycle of InfectionDocumento7 pagineLesson Plan Cycle of InfectionJeanette Bonifacio CorpuzNessuna valutazione finora
- Guidance For Dealing With COVID-19 Under FIDIC and NECDocumento24 pagineGuidance For Dealing With COVID-19 Under FIDIC and NECyoniNessuna valutazione finora
- Microbio PDFDocumento17 pagineMicrobio PDFHernandez IanNessuna valutazione finora
- PerioPruv The Next Big Thing - PPD Nov 11Documento1 paginaPerioPruv The Next Big Thing - PPD Nov 11Carolyn WilkinsonNessuna valutazione finora
- Infectious Disease Medical Behavioral Screens AmendedDocumento6 pagineInfectious Disease Medical Behavioral Screens AmendedHengkyNessuna valutazione finora