Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- 14 Talking The OTalkDocumento1 pagina14 Talking The OTalkBill WongNessuna valutazione finora
- Blueprint For Telerehab GuidelinesDocumento4 pagineBlueprint For Telerehab GuidelinesBill WongNessuna valutazione finora
- Smart Technology - Gentry - CompressedDocumento38 pagineSmart Technology - Gentry - CompressedBill WongNessuna valutazione finora
- Invited Commentary On "Sensory Sensitivities of Gifted Children"Documento5 pagineInvited Commentary On "Sensory Sensitivities of Gifted Children"Bill WongNessuna valutazione finora
- AOTA Telerehabilitation Position PaperDocumento8 pagineAOTA Telerehabilitation Position PaperBill WongNessuna valutazione finora
- Telerehab Practice AreasDocumento2 pagineTelerehab Practice AreasBill WongNessuna valutazione finora
- VOIP For Telerehabillitation - A Risk AnalysisDocumento12 pagineVOIP For Telerehabillitation - A Risk AnalysisBill WongNessuna valutazione finora
- VOIP For Telerehabillitation - A Risk AnalysisDocumento12 pagineVOIP For Telerehabillitation - A Risk AnalysisBill WongNessuna valutazione finora
- Gentry HandoutsDocumento10 pagineGentry HandoutsBill WongNessuna valutazione finora
- Gentry HandoutsDocumento10 pagineGentry HandoutsBill WongNessuna valutazione finora
- Health Literacy in The Autism ContextDocumento39 pagineHealth Literacy in The Autism ContextBill WongNessuna valutazione finora
- Live Strong, Learn Strong, Sierra Strong2012Documento34 pagineLive Strong, Learn Strong, Sierra Strong2012Bill WongNessuna valutazione finora
- Live Strong, Learn Strong, Sierra Strong2012Documento34 pagineLive Strong, Learn Strong, Sierra Strong2012Bill WongNessuna valutazione finora
- 30 Brownstone SchoenDocumento28 pagine30 Brownstone SchoenBill WongNessuna valutazione finora
- Nature of Motor Imitation Problems in School-Aged Boys With Autism: A Motor or A Cognitive Problem?Documento17 pagineNature of Motor Imitation Problems in School-Aged Boys With Autism: A Motor or A Cognitive Problem?Bill WongNessuna valutazione finora
- Sleep Problems in Autism: Prevalence, Cause, and InterventionDocumento7 pagineSleep Problems in Autism: Prevalence, Cause, and InterventionBill WongNessuna valutazione finora
- Take Time To Listen: A First Step Toward Collaborative Transition PlanningDocumento3 pagineTake Time To Listen: A First Step Toward Collaborative Transition PlanningBill WongNessuna valutazione finora
- Student Track MorrisDocumento9 pagineStudent Track MorrisBill WongNessuna valutazione finora
- Bill's 2012 OTAC Presentation FinalDocumento62 pagineBill's 2012 OTAC Presentation FinalBill WongNessuna valutazione finora
- Dinnertime and Bedtime Routines and Rituals in Families With A Young Child With An Autism Spectrum DisorderDocumento10 pagineDinnertime and Bedtime Routines and Rituals in Families With A Young Child With An Autism Spectrum DisorderBill WongNessuna valutazione finora
- Occupational Patterns of Parents of Children With ASDDocumento17 pagineOccupational Patterns of Parents of Children With ASDBill WongNessuna valutazione finora
- Oral Care and Sensory Sensitivities in Children With Autism Spectrum DisordersDocumento9 pagineOral Care and Sensory Sensitivities in Children With Autism Spectrum DisordersBill WongNessuna valutazione finora
- Heather Miller Kuhaneck Sarah Yeaton Deb WidmanDocumento15 pagineHeather Miller Kuhaneck Sarah Yeaton Deb WidmanBill WongNessuna valutazione finora
- CTRL/7c/e/910/86f/6e9/422/499/9fc/055/904/ee1/e8/a662 1Documento3 pagineCTRL/7c/e/910/86f/6e9/422/499/9fc/055/904/ee1/e8/a662 1Bill WongNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Hunger Games ThesisDocumento97 pagineHunger Games ThesisLadius PromtheusNessuna valutazione finora
- A Study On Vocational Needs of Inmates of Government Childrens Homes in KeralaDocumento11 pagineA Study On Vocational Needs of Inmates of Government Childrens Homes in KeralaIJAR JOURNALNessuna valutazione finora
- Uwrt 1104 Topic ProposalDocumento4 pagineUwrt 1104 Topic Proposalapi-384869872Nessuna valutazione finora
- UTS Material SelfDocumento16 pagineUTS Material SelfGia Espinosa Ocbeña0% (1)
- God's For-BEAR-ance With Bullies-Condensed VersionDocumento205 pagineGod's For-BEAR-ance With Bullies-Condensed VersionPatricia BackoraNessuna valutazione finora
- Attention-Deficit Hyperactivity Disorder: A Handbook For Diagnosis and Treatment (4th Ed.)Documento4 pagineAttention-Deficit Hyperactivity Disorder: A Handbook For Diagnosis and Treatment (4th Ed.)JANICE JOSEPHINE TJONDROWIBOWO 11-S3Nessuna valutazione finora
- Preliminary Business Studies - Mindmap OverviewDocumento1 paginaPreliminary Business Studies - Mindmap OverviewgreycouncilNessuna valutazione finora
- Repairing Damaged Family RelationshipsDocumento2 pagineRepairing Damaged Family RelationshipsGautam Chandgothia50% (2)
- 12b. The Central Auditory PathwayDocumento2 pagine12b. The Central Auditory PathwayShivan UmamaheswaranNessuna valutazione finora
- The Magic Cafe Forums - Mentalism IncorporatedDocumento7 pagineThe Magic Cafe Forums - Mentalism IncorporatedHendri AlamNessuna valutazione finora
- Dissertation On Consumer BehaviorDocumento6 pagineDissertation On Consumer BehaviorPayForPaperMurfreesboro100% (1)
- English 1201 2013-14 LHDocumento2 pagineEnglish 1201 2013-14 LHapi-237753417Nessuna valutazione finora
- Challenges in Leadership Development 2023Documento26 pagineChallenges in Leadership Development 2023Girma KusaNessuna valutazione finora
- Measuring Customer Satisfaction at 5 Floor Beauty SalonDocumento40 pagineMeasuring Customer Satisfaction at 5 Floor Beauty SalonIsha MohantyNessuna valutazione finora
- Media Sociology-Fall 2019 - MIDTERM ExamDocumento24 pagineMedia Sociology-Fall 2019 - MIDTERM ExamNourah BaselNessuna valutazione finora
- A Conference Schedule Reading Comprehension British CouncilDocumento3 pagineA Conference Schedule Reading Comprehension British CouncilRichard StrangeNessuna valutazione finora
- Stephen Edred Flowers - Contra Templum (2001)Documento12 pagineStephen Edred Flowers - Contra Templum (2001)Various Tings100% (1)
- Animal Love: Exercise 1: Are The Following Statements True or False?Documento2 pagineAnimal Love: Exercise 1: Are The Following Statements True or False?Andrea MeijomilNessuna valutazione finora
- Lifelong Learning Notes: From LIFELONG LEARNING AND HIGHER EDUCATION Christopher K Knapper, Arthur J CropleyDocumento3 pagineLifelong Learning Notes: From LIFELONG LEARNING AND HIGHER EDUCATION Christopher K Knapper, Arthur J CropleyGe VergaNessuna valutazione finora
- Test 1 - Identification (2 Points Each) : Bugo National High School-SHSDocumento2 pagineTest 1 - Identification (2 Points Each) : Bugo National High School-SHSNamja Ileum Ozara GaabucayanNessuna valutazione finora
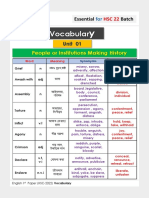
- Vocabulary HSC 22 PDFDocumento28 pagineVocabulary HSC 22 PDFMadara Uchiha83% (6)
- ANTENOR 10-Pages PublishableDocumento10 pagineANTENOR 10-Pages PublishableMary Ann AntenorNessuna valutazione finora
- Helen Milner Review: International Theories of Cooperation Amongs NationsDocumento32 pagineHelen Milner Review: International Theories of Cooperation Amongs NationsLena LeNessuna valutazione finora
- War Thesis StatementsDocumento8 pagineWar Thesis StatementsHelpPaperRochester100% (2)
- Literacy UnitDocumento8 pagineLiteracy Unitapi-463933980Nessuna valutazione finora
- The Many Questions Surrounding Jan Van Eyck's Arnolfini PortraitDocumento6 pagineThe Many Questions Surrounding Jan Van Eyck's Arnolfini Portraitapi-377336200Nessuna valutazione finora
- Jerrold Levinson-Contemplating Art-Oxford University Press Inc (2006)Documento432 pagineJerrold Levinson-Contemplating Art-Oxford University Press Inc (2006)Guillermo Jaimes BenítezNessuna valutazione finora
- Mext Research NotesDocumento5 pagineMext Research Noteskimmandy36100% (2)
- Biting PolicyDocumento1 paginaBiting PolicyJulie PeaseyNessuna valutazione finora
- Afterword The Human in The Posthuman PDFDocumento5 pagineAfterword The Human in The Posthuman PDFmonja777Nessuna valutazione finora