OBSERVATION
Right Orbitofrontal Tumor With Pedophilia
Symptom and Constructional Apraxia Sign
Jeffrey M. Burns, MD; Russell H. Swerdlow, MD
Background: Orbitofrontal abnormalities are associ- deficits, including agraphia, resolved following tumor
ated with poor impulse control, altered sexual behavior, resection.
and sociopathy.
Conclusions: For patients with acquired sociopathy and
Objective: To describe a patient with acquired pedo- paraphilia, an orbitofrontal localization requires consid-
philia and a right orbitofrontal tumor who was unable to eration. This case further illustrates that constructional
inhibit sexual urges despite preserved moral knowledge. apraxia can arise from right prefrontal lobe dysfunc-
tion. Agraphia may represent a manifestation of con-
Design: Case report. structional apraxia in the absence of aphasia and ideo-
motor apraxia.
Results: The patient displayed impulsive sexual behav-
ior with pedophilia, marked constructional apraxia, and
agraphia. The behavioral symptoms and constructional Arch Neurol. 2003;60:437-440
T
HE ORBITOFRONTAL cortex to purveyors of child pornography. He also
contributes to moral- solicited prostitution at “massage par-
knowledge acquisition and lors,” which he had not previously done.
social integration.1,2 Adult- The patient went to great lengths to
acquired orbitofrontal dam- conceal his activities because he felt that
age may diminish impulse control and can they were unacceptable. However, he con-
be associated with sociopathic behavior.3-5 tinued to act on his sexual impulses, stat-
We describe a 40-year-old man who was ing that “the pleasure principle over-
treated with medroxyprogesterone acetate rode” his urge restraint. He began making
and a 12-step program for new-onset pe- subtle sexual advances toward his pre-
dophilia. He was subsequently diagnosed as pubescent stepdaughter, which he was able
having a right orbitofrontal tumor. At the to conceal from his wife for several weeks.
time of tumor discovery, his neurologic ex- Only after the stepdaughter informed the
amination results were notable for a pau- wife of the patient’s behavior did she dis-
city of sensorimotor signs, marked con- cover with further investigation his emerg-
structional apraxia, and agraphia. ing preoccupation with pornography, and
child pornography in particular. The pa-
REPORT OF A CASE tient was legally removed from the home,
diagnosed as having pedophilia, and pre-
A 40-year-old, right-handed man in an oth- scribed medroxyprogesterone. He was
erwise normal state of health developed an found guilty of child molestation and was
increasing interest in pornography, in- ordered by a judge to either undergo in-
cluding child pornography. He had a pre- patient rehabilitation in a 12-step pro-
existing strong interest in pornography gram for sexual addiction or go to jail. De-
dating back to adolescence, although he spite his strong desire to avoid prison, he
denied a previous attraction to children could not restrain himself from soliciting
and had never experienced related social sexual favors from staff and other clients
or marital problems as a consequence. at the rehabilitation center and was ex-
Throughout the year 2000, he acquired an pelled. The evening before his prison sen-
expanding collection of pornographic tencing, he came to the University of Vir-
From the Department of magazines and increasingly frequented In- ginia Hospital (Charlottesville) emergency
Neurology, University of ternet pornography sites. Much of this pru- department complaining of a headache. A
Virginia Health System, rient material emphasized children and nonphysiologic cause was suspected, and
Charlottesville. adolescents and was specifically targeted the psychiatry service admitted him with
(REPRINTED) ARCH NEUROL / VOL 60, MAR 2003 WWW.ARCHNEUROL.COM
437
Downloaded from www.archneurol.com on May 31, 2011
©2003 American Medical Association. All rights reserved.
A B C
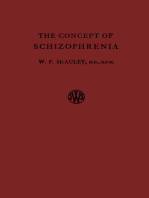
Figure 1. Magnetic resonance imaging scans at the time of initial neurologic evaluation: T1 sagittal (A), contrast-enhanced coronal (B), and contrast-enhanced
axial (C) views. In A and B, the tumor mass extends superiorly from the olfactory groove, displacing the right orbitofrontal cortex and distorting the dorsolateral
prefrontal cortex. The tumor is capped by a large cystic portion.
a diagnosis of pedophilia, not otherwise specified, after with the figure copy test (Figure 2A). Simultanagnosia was
he expressed suicidal ideation and a fear that he would absent. Although spontaneous language output, repeti-
rape his landlady. The day after his admission he com- tion, comprehension, and reading skills were intact, his writ-
plained of balance problems, and a neurologic consul- ing was illegible (Figure 2B). The patient was able to spell,
tation was obtained. and prosody was normal. During 1-minute intervals he
The patient’s medical history was notable for a closed named 5, 7, and 5 words beginning with C, F, and L, re-
head injury 16 years earlier that was associated with a spectively (bottom of first percentile). He named 11 ani-
2-minute loss of consciousness and no apparent neuro- mals during 1 minute. He verbally shifted between letter
logical sequelae, a 2-year history of migraines, and hyper- and number sets, conceptualized, performed sequential
tension. He was without a previous psychiatric or devel- hand movements, and inhibited motor responses on the
opmental history and had exhibited no prior deviant sexual Luria go–no go test.7 He was without ideomotor apraxia.
behavior. Medications included fluoxetine hydrochlo- Results of olfactory testing appeared normal because the
ride, amlodipine besylate, metoclopramide hydrochloride patient correctly identified peanut butter and coffee by scent.
(for nausea), and medroxyprogesterone acetate at a dose He performed normally on a task of visuoperception (Luria
of 10 mg/d. There was no family history of psychiatric dis- figure-ground analysis8).
ease. He had worked as a corrections officer prior to com- Histopathologic examination revealed a hemangio-
pleting a master’s degree in education in 1998, at which pericytoma. Several days after tumor resection, the pa-
time he became a schoolteacher. He was currently in his tient’s walking and bladder control improved. He suc-
second marriage, which prior to his developing sexual pre- cessfully participated in a Sexaholics Anonymous program.
occupations had been stable for 2 years. Seven months later, he was believed not to pose a threat
During a neurologic examination, he solicited female to his stepdaughter and returned home. In October 2001,
team members for sexual favors. He was unconcerned that he developed a persistent headache and began secretly
he had urinated on himself. He was slow to initiate leftward collecting pornography again. Magnetic resonance im-
saccades and had mild left nasolabial fold flattening with- aging showed tumor regrowth, and re-resection was ac-
out facial weakness. Appendicular tone was increased bi- complished in February 2002.
laterally. There was no neglect. Abnormal glabellar, snout, Two days after this surgery, his examination results
and palmomental responses were present. The patient’s gait were notable only for a slightly decreased left nasolabial
was wide based, and as he walked, his step length dimin- fold. His Mini-Mental State Examination score was 30 of
ished and side-to-side titubation occurred. 30. Results of clock-drawing and figure copy tests were nor-
Magnetic resonance imaging revealed an enhancing mal (Figure 2C), and his writing was legible (Figure 2D).
anterior fossa skull base mass that displaced the right or- During 1-minute intervals he named 18, 13, and 9 words
bitofrontal lobe (Figure 1). Prior to resection (Decem- beginning with C, F, and L, respectively (51st percentile).
ber 2000), bedside neurologic testing found the patient alert He named 26 animals during 1 minute and a digit span of
and completely oriented. He scored 25 of 30 on the Fol- 8 going forward and 5 in reverse.
stein Mini-Mental State Examination,6 missing points for
delayed recall, impaired copy (Figure 2A), and an inabil- COMMENT
ity to write a legible sentence (Figure 2B). His memory, how-
ever, was intact according to a 16-item test of enhanced cued The orbitofrontal cortex is involved in the regulation of
recall on which he freely retrieved 6 objects and the re- social behavior. Lesions acquired very early in life im-
maining 10 with cues. He named the previous 5 presi- pede social- and moral-knowledge acquisition, which may
dents. He was able to state digit spans of 7 going forward result in poor judgment, reduced impulse control, and so-
and 4 in reverse. On the clock-drawing test, he exhibited ciopathy.2 A similar acquired sociopathy occurs with adult-
marked constructional apraxia, and this did not improve onset damage, but previously established moral develop-
(REPRINTED) ARCH NEUROL / VOL 60, MAR 2003 WWW.ARCHNEUROL.COM
438
Downloaded from www.archneurol.com on May 31, 2011
©2003 American Medical Association. All rights reserved.
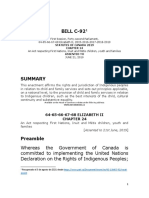
Clock
(Time = 8:20)
Figure 2. Constructional apraxia and pseudodysgraphia in our patient with a right orbitofrontal tumor. A, Impaired copy drawing and free drawing at the initial
evaluation. B, Pseudodysgraphia at the initial evaluation. C, Resolution of constructional apraxia after tumor resection. D, Resolution of pseudodysgraphia after
tumor resection.
ment is preserved. Nevertheless, poor impulse regulation tual performance on Luria figure-ground analysis suggest
leads to bad judgment and sociopathic behavior.3,4 Our pa- relatively intact parietal visuospatial function. Construc-
tient developed paraphilia late in his fourth decade and tional apraxia likely resulted from an inability to ex-
met the criteria for pedophilia according to the Diagnos- ecute the drawing task rather than a parietal-based vi-
tic and Statistical Manual of Mental Disorders, Fourth Edi- suospatial failure.
tion.9 His symptoms resolved with the excision of a right Constructional apraxia is classically associated with
orbitofrontal hemangiopericytoma, further establishing cau- parieto-occipital damage and represents a functional con-
sality. The orbitofrontal disruption likely exacerbated a pre- sequence of visuospatial dysfunction.11 It has also been
existing interest in pornography, manifesting as sexual de- reported to occur with frontal lesions.12 Constructional
viancy and pedophilia. To our knowledge, this is the first apraxia in this patient likely arose from dysfunction of
description of pedophilia as a specific manifestation of or- the dorsolateral prefrontal cortex or its connections, al-
bitofrontal syndrome. though precise localization is difficult given the tumor’s
Bedside orbitofrontal lobe assessments have low sen- size and mass effect. Regardless, the patient’s intact
sitivity. Anosmia is occasionally noted10 but was not pres- memory retrieval, working memory, set shifting, and se-
ent in our patient. Urinary incontinence, gait ataxia, fron- quencing abilities indicate that dorsolateral prefrontal dys-
tal release signs, and word generation impairment function was not pervasive. We do not know if construc-
(especially on controlled oral word association) are con- tional apraxia would have manifested from a similar
sistent with general prefrontal lesion localization. Se- dominant-sided lesion. Interestingly, frontal degenera-
vere constructional apraxia on both free-drawing and tion syndromes are associated with early decline of the
copy-drawing tests was an unexpected examination find- orbitofrontal lobes and early preservation of drawing abili-
ing that is most often attributable to parietal dysfunc- ties.13,14 Our findings emphasize that extensive right or-
tion. Absent simultanagnosia and normal visuopercep- bitofrontal damage can produce constructional apraxia.
(REPRINTED) ARCH NEUROL / VOL 60, MAR 2003 WWW.ARCHNEUROL.COM
439
Downloaded from www.archneurol.com on May 31, 2011
©2003 American Medical Association. All rights reserved.
Our patient exhibited severe agraphia that resolved cult for orbitofrontal-damaged subjects to restrain their
with resection of his anterior fossa tumor. Although agraphia exploration of the riskier, disadvantageous decks.
is typically a disorder of language associated with domi- In summary, signs of orbitofrontal lobe dysfunc-
nant inferior parietal lobe abnormalities, it can be associ- tion are often subtle. Physicians can overlook even large
ated with visuospatial deficits, limb apraxia, and sensori- orbitofrontal lesions in patients with acquired sociopa-
motor deficits.15 His agraphia is notable given the absence thy if not appropriately vigilant. Acquired sociopathy with
of limb apraxia, aphasia, and significant sensorimotor defi- concomitant constructional apraxia and pseudodys-
cits. It likely represents a distinct manifestation of his over- graphia but not simultanagnosia could indicate the pres-
all constructional apraxia. Demonstrating a preservation ence of right orbitofrontal dysfunction.
of typing ability could have corroborated this hypothesis,
but unfortunately this was not attempted prior to his tu- Submitted for publication June 13, 2002; final revision re-
mor resection. Occasionally, agraphia has been reported ceived September 23, 2002; accepted September 23, 2002.
with prefrontal lesions,16 although the mechanism for such Author contributions: Study concept and design (Dr
deficits is unclear. Agraphia resulting from constructional Swerdlow); acquisition of data (Dr Swerdlow); analysis and
apraxia is perhaps best considered pseudodysgraphia. interpretation of data (Drs Burns and Swerdlow); drafting
Orbitofrontal lesion research suggests that socio- of the manuscript (Drs Burns and Swerdlow); critical revi-
pathic behavior results from a loss of impulse control rather sion of the manuscript for important intellectual content (Dr
than a loss of moral knowledge.3,4 Functional magnetic reso- Swerdlow); administrative, technical, and material support
nance imaging studies indicate that orbitofrontal, dorso- (Drs Burns and Swerdlow); study supervision (Dr Swerdlow).
lateral prefrontal, and subcortical limbic structures are in- Corresponding author and reprints: Russell H. Swerd-
volved in behavioral self-regulation and response inhibition, low, MD, Box 800394, Department of Neurology, Univer-
including the conscious regulation of sexual urges.17 Our sity of Virginia Health System, 1 Hospital Dr, Charlottes-
patient could not refrain from acting on his pedophilia de- ville, VA 22908 (e-mail: rhs7e@virginia.edu).
spite the awareness that this behavior was inappropriate.
The somatic marker hypothesis attempts to provide a physi-
ologic explanation for this phenomenon.5 The orbitofron- REFERENCES
tal cortex receives afferents from the sensory cortex, amyg-
dala, and hippocampus. It in turn projects to brainstem 1. Eslinger PJ, Damasio AR. Severe disturbance of higher cognition after bilateral
frontal lobe ablation: patient EVR. Neurology. 1985;35:1731-1741.
autonomic nuclei. Therefore, the orbitofrontal lobes play 2. Anderson SW, Bechara A, Damasio H, Tranel D, Damasio AR. Impairment of so-
a role in generating the autonomic responses that typify a cial and moral behavior related to early damage in human prefrontal cortex. Nat
variety of emotions. The cortex subsequently attaches a feel- Neurosci. 1999;2:1032-1037.
3. Saver JL, Damasio AR. Preserved access and processing of social knowledge in
ing, or somatic marker, to the emotional response; this a patient with acquired sociopathy due to ventromedial frontal damage. Neuro-
higher-order interpretation guides behavioral response pat- psychologia. 1991;29:1241-1249.
4. Blair RJR, Cipolotti L. Impaired social response reversal: a case of acquired so-
terns to environmental stimuli. Disruption of this system ciopathy. Brain. 2000;123:1122-1141.
can result in decision making that emphasizes immediate 5. Bechara A, Damasio H, Damasio AR. Emotion, decision making and the orbito-
reward rather than long-term gain, impairing the subject’s frontal cortex. Cereb Cortex. 2000;10:295-307.
6. Folstein MF, Folstein SF, McHugh PR. “Mini-mental state”: a practical method
ability to appropriately navigate social situations. for grading the cognitive state of patients for the clinician. J Psychiatric Res. 1975;
Because prompt surgical intervention was clini- 12:189-198.
cally indicated, the neuropsychological evaluation was 7. Drewe EA. Go-no go learning after frontal lobe lesions in humans. Cortex. 1975;
11:8-16.
limited to the bedside. Although a fairly comprehensive 8. Luria AR. Neuropsychological analysis of focal brain lesions. In: Wolman BB,
assessment of the patient’s cognitive strengths and weak- ed. Handbook of Clinical Psychology. New York, NY: McGraw-Hill Co; 1965.
9. American Psychiatric Association. Diagnostic and Statistical Manual of Mental
nesses was accomplished, formal neuropsychological test- Disorders, Fourth Edition. Washington, DC: American Psychiatric Association;
ing might have allowed for a finer localization of rel- 1994.
evant signs and symptoms. It is also possible that formal 10. Sumner D. Disturbances in sense of smell and taste after head injuries. In: Vinken
P, Bruyn G, eds. Handbook of Clinical Neurology. Vol 2. New York, NY: Aca-
neuropsychological testing would have facilitated an ear- demic Press; 1976.
lier diagnosis. Tests that emphasize frontal lobe func- 11. Benton A, Tranel D. Visuoperceptual, visuospatial, and visuoconstructive disor-
tions, such as the Stroop Interference Test18 and Wis- ders. In: Heilman KM, Valenstein E, eds. Clinical Neuropsychology. New York,
NY: Oxford University Press; 1993:165-213.
consin Card Sorting Test,19 are sensitive indicators of 12. Benton AL. Differential behavioral effects in frontal lobe disease. Neuropsycho-
frontal lobe dysfunction. It is unfortunate that data from logia. 1968;6:53-60.
13. Rhaman S, Sahakian BJ, Hodges JR, Rogers RD, Robbins TW. Specific cogni-
such testing could not be obtained. In addition to these tive deficits in mild frontal variant frontotemporal dementia. Brain. 1999;122:
instruments, neuropsychological testing that is both sen- 1469-1493.
sitive and specific for orbitofrontal dysfunction has re- 14. Miller BL, Ikonte C, Ponton M, et al. A study of the Lund-Manchester research
criteria for frontotemporal dementia: clinical and single-photon emission CT cor-
cently been developed. The Iowa Gambling Task20 re- relations. Neurology. 1997;48:937-942.
quires the subject to select cards from 4 decks, and each 15. Roeltgen DP. Agraphia. In: Heilman KM, Valenstein E, eds. Clinical Neuropsy-
card selected incurs either a financial gain or financial chology. New York, NY: Oxford University Press; 1993:63-89.
16. Rosselli M, Ardila A. Spatial agraphia. Brain Cogn. 1993;22:137-147.
loss. Cards from 2 of the decks will occasionally result 17. Beauregard M, Levesque J, Bourgouin P. Neural correlates of conscious self-
in a substantial payoff, but choosing from these decks regulation of emotion. J Neurosci. 2001;21:RC165.
18. Stroop JR. Studies of interference in serial verbal reactions. J Exp Psychol. 1935;
ultimately results in a net loss. The other 2 decks are char- 18:643-662.
acterized by more conservative payoffs and penalties. Play- 19. Milner B. Effects of different brain lesions on card sorting. Arch Neurol. 1963;
ing these decks results in a net financial gain. This para- 9:90-100.
20. Bechara A, Damasio AR, Damasio H, Anderson SW. Insensitivity to future con-
digm can distinguish individuals with orbitofrontal sequences following damage to human prefrontal cortex. Cognition. 1994;50:
dysfunction from control individuals because it is diffi- 7-15.
(REPRINTED) ARCH NEUROL / VOL 60, MAR 2003 WWW.ARCHNEUROL.COM
440
Downloaded from www.archneurol.com on May 31, 2011
©2003 American Medical Association. All rights reserved.
Potrebbero piacerti anche
- Anorectal Autoeroticism: A Case ReportDocumento3 pagineAnorectal Autoeroticism: A Case ReportdavockNessuna valutazione finora
- Delong 1981 en Cefalo Pat I ADocumento4 pagineDelong 1981 en Cefalo Pat I A__aguNessuna valutazione finora
- Evaluating The Child For Sexual Abuse PDFDocumento10 pagineEvaluating The Child For Sexual Abuse PDFEduardo LuayonNessuna valutazione finora
- ComorbilidadesDocumento3 pagineComorbilidadesMiguel NadalNessuna valutazione finora
- Garcia 2010Documento7 pagineGarcia 2010Margarida SolizNessuna valutazione finora
- Case Study For Paranoid SchizophreniaDocumento30 pagineCase Study For Paranoid SchizophreniaCherubim Lei DC FloresNessuna valutazione finora
- Penile Self-AmputationDocumento3 paginePenile Self-Amputationgion.nandNessuna valutazione finora
- Hypersexualityor Alteredsexualpreferencefollowing Brain InjuryDocumento8 pagineHypersexualityor Alteredsexualpreferencefollowing Brain Injurysara_vonNessuna valutazione finora
- SchizophreniaDocumento12 pagineSchizophreniasoha nooraniNessuna valutazione finora
- Mother and Daughter With Adolescent-Onset Severe Frontal Lobe Dysfunction and EpilepsyDocumento7 pagineMother and Daughter With Adolescent-Onset Severe Frontal Lobe Dysfunction and EpilepsyJesús Aldair Lozano SuárezNessuna valutazione finora
- Sexsomnia-A New Parasomnia?: Original ResearchDocumento7 pagineSexsomnia-A New Parasomnia?: Original Researchjesus malvaezNessuna valutazione finora
- NEJMDocumento9 pagineNEJMbernard surbaktiNessuna valutazione finora
- The Wrong Answer: by Harold D. Foster, PHD © 2003Documento6 pagineThe Wrong Answer: by Harold D. Foster, PHD © 2003JOSH USHERNessuna valutazione finora
- The Accuracy of 2D Ultrasound Prenatal Sex Determination: Original ArticleDocumento6 pagineThe Accuracy of 2D Ultrasound Prenatal Sex Determination: Original ArticledrIndah NoviantyNessuna valutazione finora
- Human Kluver-Bucy: SyndromeDocumento6 pagineHuman Kluver-Bucy: SyndromeFlorencia RubioNessuna valutazione finora
- Strub 1989Documento4 pagineStrub 1989mgobiNessuna valutazione finora
- Distant IntentioDocumento12 pagineDistant IntentioZzNessuna valutazione finora
- Curses, Madness, and MefloquineDocumento3 pagineCurses, Madness, and MefloquineChristopher DoddNessuna valutazione finora
- Art 3Documento26 pagineArt 3Clinica MonserratNessuna valutazione finora
- 25th European Congress of Psychiatry / European Psychiatry 41S (2017) S303-S364 S331Documento1 pagina25th European Congress of Psychiatry / European Psychiatry 41S (2017) S303-S364 S331shreya DahalNessuna valutazione finora
- Paranoid Schizophrenia Case StudyDocumento33 pagineParanoid Schizophrenia Case StudyCherubim Lei DC Flores50% (4)
- Kanner Problems of Nosology and Psychodynamics 2oexnb5Documento11 pagineKanner Problems of Nosology and Psychodynamics 2oexnb5Aleffe Gomes MendesNessuna valutazione finora
- Sexual Obsessions in A Patient With SchizophreniaDocumento5 pagineSexual Obsessions in A Patient With SchizophreniaSteph TgdNessuna valutazione finora
- NCMH Case Study-GiaDocumento57 pagineNCMH Case Study-GiaBorlongan PaulineNessuna valutazione finora
- Cognitive Therapy Versus Medication - For Depression - Treatment Outcomes - and Neural MechanismsDocumento9 pagineCognitive Therapy Versus Medication - For Depression - Treatment Outcomes - and Neural MechanismsComercial 03Nessuna valutazione finora
- ArticleDocumento15 pagineArticleEmily Gisset Delgado JaimesNessuna valutazione finora
- Cariotipo X Fragil y 47, XXX PDFDocumento6 pagineCariotipo X Fragil y 47, XXX PDFLìzeth RamìrezNessuna valutazione finora
- Patient EVRDocumento12 paginePatient EVRJorge CastilloNessuna valutazione finora
- Psychiatric History and Mental Status ExaminationDocumento4 paginePsychiatric History and Mental Status Examinationallen cabasagNessuna valutazione finora
- Inceput Articol DelceaDocumento9 pagineInceput Articol DelceaAmalia BondreaNessuna valutazione finora
- AbnormalDocumento3 pagineAbnormalmacio853Nessuna valutazione finora
- Compulsive Masturbation Treated With Fluvoxamine-A Case StudyDocumento3 pagineCompulsive Masturbation Treated With Fluvoxamine-A Case StudyNisha SharmaNessuna valutazione finora
- Hypersexuality in DementiaDocumento8 pagineHypersexuality in DementiaElton MatsushimaNessuna valutazione finora
- Forcen. Schizencephaly and BDPDocumento1 paginaForcen. Schizencephaly and BDPMarcela-Felicia BalanNessuna valutazione finora
- Persistent Delusional DisorderDocumento4 paginePersistent Delusional DisorderShandy PutraNessuna valutazione finora
- Decoding Schizophrenia PDFDocumento8 pagineDecoding Schizophrenia PDFAvengingBrain100% (2)
- Lilliputian Hallucinations Understanding A Strange PhenomenonDocumento4 pagineLilliputian Hallucinations Understanding A Strange PhenomenonMGotts100% (1)
- Bataan Case EditedDocumento21 pagineBataan Case EditedCham Rafaela ConeseNessuna valutazione finora
- 1 s2.0 S1878875020315084 MainDocumento6 pagine1 s2.0 S1878875020315084 MainilonaskorinNessuna valutazione finora
- Late Onset SchizophreniaDocumento6 pagineLate Onset SchizophreniaVijay MgNessuna valutazione finora
- Behavioral Genetics: The Clash of Culture and BiologyDa EverandBehavioral Genetics: The Clash of Culture and BiologyNessuna valutazione finora
- 22childhood Masturbation Simulating Epileptic Seizures A Report of Two Cases and Review of The LiteratureDocumento3 pagine22childhood Masturbation Simulating Epileptic Seizures A Report of Two Cases and Review of The Literaturesam_mad00100% (1)
- Cu 3 Week 3Documento3 pagineCu 3 Week 3Maica LectanaNessuna valutazione finora
- Anino NG KahaponDocumento5 pagineAnino NG KahaponFrancis CervantesNessuna valutazione finora
- Análisis Neuropsicológico de Un Caso Con Anosognosia: Revista Chilena de Neuro-Psiquiatria October 2020Documento7 pagineAnálisis Neuropsicológico de Un Caso Con Anosognosia: Revista Chilena de Neuro-Psiquiatria October 2020EDUARDO ALEXIS NOVOA IBARRANessuna valutazione finora
- Demencia SemanticaDocumento5 pagineDemencia SemanticaJesus DecepcionadoNessuna valutazione finora
- Case Pres-Banag Laum SuperfinaleDocumento46 pagineCase Pres-Banag Laum SuperfinaleAyen FornollesNessuna valutazione finora
- NCP Neuro 0194Documento5 pagineNCP Neuro 0194Fiaz medicoNessuna valutazione finora
- Bugs, Bowels, and Behavior: The Groundbreaking Story of the Gut-Brain ConnectionDa EverandBugs, Bowels, and Behavior: The Groundbreaking Story of the Gut-Brain ConnectionNessuna valutazione finora
- Role of The Family During AdolescenceDocumento2 pagineRole of The Family During AdolescenceDelia KrisnasariNessuna valutazione finora
- A Case of Inappropriate Sexual Behaviour in Mixed DementiaDocumento2 pagineA Case of Inappropriate Sexual Behaviour in Mixed DementiavickyreyeslucanoNessuna valutazione finora
- Lectura de Trabajo 1 InglesDocumento7 pagineLectura de Trabajo 1 InglesRaul CelesteNessuna valutazione finora
- Day 1 - SCHIZOPHRENIA DISORDERDocumento16 pagineDay 1 - SCHIZOPHRENIA DISORDERMaria Charis Anne IndananNessuna valutazione finora
- NCM 105 Rle Case 1 BasigDocumento17 pagineNCM 105 Rle Case 1 BasigMaria Charis Anne IndananNessuna valutazione finora
- 268 Price, Brain, 1990Documento12 pagine268 Price, Brain, 1990MaríaJesúsOpazoPintoNessuna valutazione finora
- Multiple Paraphilic Diagnoses Among Sex OffendersDocumento16 pagineMultiple Paraphilic Diagnoses Among Sex OffendersRaphael Moro Villas BoasNessuna valutazione finora
- Assessment of Knowledge, Attitude Practice, Commmunity Based Study'Documento8 pagineAssessment of Knowledge, Attitude Practice, Commmunity Based Study'Leonhardt RowikaNessuna valutazione finora
- Case Study-A Patient With Severe DelusionsDocumento3 pagineCase Study-A Patient With Severe DelusionsKrizzia Louise B. CabreraNessuna valutazione finora
- Palmer Martinson RevisitedDocumento20 paginePalmer Martinson RevisitedFrancisco EstradaNessuna valutazione finora
- Hanks Family NamesDocumento25 pagineHanks Family NamesFrancisco EstradaNessuna valutazione finora
- Besson The Principle of Non-Discrimination in CRCDocumento33 pagineBesson The Principle of Non-Discrimination in CRCFrancisco EstradaNessuna valutazione finora
- California Court Frantic, Inc. (Metallica) v. Certain Underwriters at Lloyd's, LondonDocumento29 pagineCalifornia Court Frantic, Inc. (Metallica) v. Certain Underwriters at Lloyd's, LondonFrancisco EstradaNessuna valutazione finora
- Comité de La CEDAW General Recommendation 39 (2022) On The Rights of Indigenous Women and GirlsDocumento23 pagineComité de La CEDAW General Recommendation 39 (2022) On The Rights of Indigenous Women and GirlsFrancisco EstradaNessuna valutazione finora
- O'Neill Children's Rights and Children's LivesDocumento19 pagineO'Neill Children's Rights and Children's LivesFrancisco EstradaNessuna valutazione finora
- MacFarquhar When Should A Child Be Taken From His ParentsDocumento38 pagineMacFarquhar When Should A Child Be Taken From His ParentsFrancisco EstradaNessuna valutazione finora
- Trivedi, Shantal (2019) - The Harm of Child RemovalDocumento59 pagineTrivedi, Shantal (2019) - The Harm of Child RemovalFrancisco EstradaNessuna valutazione finora
- Lopatka The Rights of The Child Are UniversalDocumento6 pagineLopatka The Rights of The Child Are UniversalFrancisco EstradaNessuna valutazione finora
- Estudio NU Niños Privados de Libertad 527-594Documento68 pagineEstudio NU Niños Privados de Libertad 527-594Francisco EstradaNessuna valutazione finora
- Goldman Institutionalisation and Deinstitutionalisation of Children 2Documento28 pagineGoldman Institutionalisation and Deinstitutionalisation of Children 2Francisco EstradaNessuna valutazione finora
- McPherson Crushing Creativity The Blurred Lines Case and Its AftermathDocumento16 pagineMcPherson Crushing Creativity The Blurred Lines Case and Its AftermathFrancisco EstradaNessuna valutazione finora
- Bill C-92Documento16 pagineBill C-92Francisco EstradaNessuna valutazione finora
- Case X V BulgariaDocumento100 pagineCase X V BulgariaFrancisco EstradaNessuna valutazione finora
- Case-Law of The European Court of Human Rights Related To Child Rights, Role of The Families and Alternative Care 1Documento9 pagineCase-Law of The European Court of Human Rights Related To Child Rights, Role of The Families and Alternative Care 1Francisco EstradaNessuna valutazione finora
- Draft General Comment No. 25Documento20 pagineDraft General Comment No. 25Francisco EstradaNessuna valutazione finora
- Nicholson v. ScoppettaDocumento24 pagineNicholson v. ScoppettaFrancisco EstradaNessuna valutazione finora
- BURNS Child Removal Decision-Making Systems in Ireland Law, Policy andDocumento34 pagineBURNS Child Removal Decision-Making Systems in Ireland Law, Policy andFrancisco EstradaNessuna valutazione finora
- Convention On The Rights of The Child: United NationsDocumento19 pagineConvention On The Rights of The Child: United NationssofiabloemNessuna valutazione finora
- White Paper On The EU Directive 2016 800Documento38 pagineWhite Paper On The EU Directive 2016 800Francisco EstradaNessuna valutazione finora
- Rights, Remedies and RepresentationDocumento44 pagineRights, Remedies and RepresentationFrancisco EstradaNessuna valutazione finora
- Pub Nietzsches Genealogy of MoralityDocumento192 paginePub Nietzsches Genealogy of MoralitySamuel Enrique Cano Patoc100% (1)
- Lit ReviewDocumento6 pagineLit ReviewMuhammad Ikhtiaruddin Asy-SyahidiNessuna valutazione finora
- fs2 - Episode 8Documento6 paginefs2 - Episode 8Jamille Nympha C. BalasiNessuna valutazione finora
- Ontological and Epistemological Foundations of Qualitative ResearchDocumento25 pagineOntological and Epistemological Foundations of Qualitative ResearchPablo Azevedo100% (1)
- T2- B107- Nguyễn Thành TâyDocumento2 pagineT2- B107- Nguyễn Thành TâyTây Nguyễn ThànhNessuna valutazione finora
- Rap RubricDocumento1 paginaRap RubricCherlyn Arias IbañezNessuna valutazione finora
- Teaching MethodsDocumento32 pagineTeaching Methodsklara klaraNessuna valutazione finora
- Science 7Documento4 pagineScience 7Yvette Marie Yaneza NicolasNessuna valutazione finora
- Reader's TheaterDocumento12 pagineReader's TheaterTeodora Ramos100% (2)
- Activity Completion Report: 1 Slac (School Learning Action Cell) SessionDocumento7 pagineActivity Completion Report: 1 Slac (School Learning Action Cell) SessionEsmeralda Aniban Rojo75% (8)
- The Brand Report CardDocumento1 paginaThe Brand Report Cardpeace makerNessuna valutazione finora
- The Postmodernist Perspective in PoliticsDocumento5 pagineThe Postmodernist Perspective in PoliticskavyaNessuna valutazione finora
- Chapter 2 Values and EthicsDocumento30 pagineChapter 2 Values and EthicsWalaa Alali100% (1)
- Cognitive Components of Social AnxietyDocumento4 pagineCognitive Components of Social AnxietyAdina IlieNessuna valutazione finora
- Engineering EthicsDocumento21 pagineEngineering Ethicssraj_4uNessuna valutazione finora
- PM1 SchizophreniaDocumento12 paginePM1 SchizophreniaShivani SharmaNessuna valutazione finora
- Food and Drink Lesson Plan 1Documento6 pagineFood and Drink Lesson Plan 1phalonnolan0% (1)
- Discuss The Free Will and Determinism DebateDocumento2 pagineDiscuss The Free Will and Determinism DebateAnonymous q55fD35fPNessuna valutazione finora
- Behavior Incident Report FormDocumento2 pagineBehavior Incident Report FormAkash RanaNessuna valutazione finora
- Sensemaking, Knowledge Creation, and Decision MakingDocumento11 pagineSensemaking, Knowledge Creation, and Decision Makingfjsvasconcellos100% (1)
- On Needing To Find Something To Worry AboutDocumento3 pagineOn Needing To Find Something To Worry AboutKyle BabcockNessuna valutazione finora
- Tree Sorting Lesson PlanDocumento3 pagineTree Sorting Lesson Planapi-478219036Nessuna valutazione finora
- Role of Teacher in A SchoolDocumento11 pagineRole of Teacher in A SchoolJay LauNessuna valutazione finora
- Ielts Writing Task 2Documento19 pagineIelts Writing Task 2Ann Study With100% (1)
- Planned ChangeDocumento36 paginePlanned ChangeSara AssiriNessuna valutazione finora
- Test Bank For Contemporary Marketing 18th by BooneDocumento33 pagineTest Bank For Contemporary Marketing 18th by Boonebettywalkertwpgakecbm100% (26)
- Reported Speech ReviewDocumento2 pagineReported Speech Reviewapi-459088986Nessuna valutazione finora
- Motivations and Attitudes in Language Learning A Literature ReviewDocumento16 pagineMotivations and Attitudes in Language Learning A Literature ReviewRiad HakimNessuna valutazione finora
- A Study of Reasons For Codeswitching in Pakistani Context: Literature ReviewDocumento10 pagineA Study of Reasons For Codeswitching in Pakistani Context: Literature ReviewwaseemNessuna valutazione finora
- What Kind of Citizen? An Analysis of The Social Studies Curriculum in TurkeyDocumento14 pagineWhat Kind of Citizen? An Analysis of The Social Studies Curriculum in TurkeyRITWIK RANJANNessuna valutazione finora