Potrebbero piacerti anche
- Principles of SurgeryDocumento87 paginePrinciples of SurgeryfiansisNessuna valutazione finora
- Septic Shock TreatmentDocumento22 pagineSeptic Shock TreatmentAdreiTheTripleA100% (1)
- Anesthesia For Patients With Diabetes Mellitus - UpToDateDocumento31 pagineAnesthesia For Patients With Diabetes Mellitus - UpToDateEduardoNessuna valutazione finora
- Management of Diabetes Mellitus in Surgical PatientsDocumento12 pagineManagement of Diabetes Mellitus in Surgical PatientsAnggoro Bayu Agung DjangkaruNessuna valutazione finora
- Thinking Like A PancreasDocumento3 pagineThinking Like A Pancreasdevabakhti100% (1)
- Evidence-Based Clinical Guidelines For InjectionDocumento68 pagineEvidence-Based Clinical Guidelines For Injectionagilen100% (1)
- Acarbose: An A-Glucosidase InhibitorDocumento14 pagineAcarbose: An A-Glucosidase Inhibitor20128139Nessuna valutazione finora
- Management Amputations : G EHE IntoDocumento15 pagineManagement Amputations : G EHE IntoDenim Embalzado MaghanoyNessuna valutazione finora
- Blunt Abdominal Injuries: Adam J Brooks and Brian J RowlandsDocumento12 pagineBlunt Abdominal Injuries: Adam J Brooks and Brian J RowlandsRajan KarmakarNessuna valutazione finora
- Partridge 2015Documento9 paginePartridge 2015ppica8111Nessuna valutazione finora
- Pharmacologic Approaches To Glycemic Treatment: Standards of Medical Care in Diabetes 2019Documento36 paginePharmacologic Approaches To Glycemic Treatment: Standards of Medical Care in Diabetes 2019AndikhaNessuna valutazione finora
- Optimal Glucose Management in The Perioperative PeriodDocumento18 pagineOptimal Glucose Management in The Perioperative PeriodJULIAN DAVID CAICEDO ROZONessuna valutazione finora
- Counseling Patients On Bariatric Surgery For ObesityDocumento6 pagineCounseling Patients On Bariatric Surgery For ObesityMohamed EssallaaNessuna valutazione finora
- Diabetes-Specific Enteral NutrDocumento14 pagineDiabetes-Specific Enteral NutrFitri WulandariNessuna valutazione finora
- Nutritional Intervention in Chronic Kidney Disease: EditorialDocumento2 pagineNutritional Intervention in Chronic Kidney Disease: EditorialDaniel DarmawanNessuna valutazione finora
- Abstracts For The Website - pdf1441898071Documento166 pagineAbstracts For The Website - pdf1441898071Radu MiricaNessuna valutazione finora
- Cummings 2017Documento8 pagineCummings 2017Ioanna Bianca HNessuna valutazione finora
- Clinician Guide Inpx LCD For Remission T2DM Toward STD Care Protocol Diabetes Manag 2019 9-Cucuzzella Hite Patterson EtalDocumento28 pagineClinician Guide Inpx LCD For Remission T2DM Toward STD Care Protocol Diabetes Manag 2019 9-Cucuzzella Hite Patterson Etaldonmd98Nessuna valutazione finora
- Albumin Guidelines UHS April 2010Documento5 pagineAlbumin Guidelines UHS April 2010dradrianramdhanyNessuna valutazione finora
- Samba Consensus For Diabetes During Ambulatory SurgeryDocumento5 pagineSamba Consensus For Diabetes During Ambulatory Surgeryabirray65Nessuna valutazione finora
- Nutrition in Gastrointestinal Cancer Patient: Intensive Care Unit RSPAD Gatot Soebroto 2021Documento16 pagineNutrition in Gastrointestinal Cancer Patient: Intensive Care Unit RSPAD Gatot Soebroto 2021Muhammad Baihaqi SiddiqNessuna valutazione finora
- Dietary Intake and Ghrelin and Leptin Changes After SleeveDocumento8 pagineDietary Intake and Ghrelin and Leptin Changes After Sleevea12345644321Nessuna valutazione finora
- Mingrone 2015Documento10 pagineMingrone 2015Ana GomezNessuna valutazione finora
- Fany Jurnal Anestesi FixDocumento16 pagineFany Jurnal Anestesi Fixwahyuni taslimNessuna valutazione finora
- Cvac 176Documento18 pagineCvac 176Helder LezamaNessuna valutazione finora
- Perioperative Blood Glucose Monitoring in The General Surgical PopulationDocumento6 paginePerioperative Blood Glucose Monitoring in The General Surgical PopulationsimscityNessuna valutazione finora
- Nutrisi in SurgeryDocumento26 pagineNutrisi in Surgeryfeby ary annasNessuna valutazione finora
- Avoiding Revascularization With Lifestyle Changes: The Multicenter Lifestyle Demonstration ProjectDocumento5 pagineAvoiding Revascularization With Lifestyle Changes: The Multicenter Lifestyle Demonstration ProjectNag Mallesh RaoNessuna valutazione finora
- Bariatric SurgeryDocumento5 pagineBariatric SurgeryMiguelito JohnsonNessuna valutazione finora
- Glucosa 2012Documento6 pagineGlucosa 2012martynbbNessuna valutazione finora
- Surgery in Morbid ObesityDocumento28 pagineSurgery in Morbid ObesityalaaNessuna valutazione finora
- Anaesthesia - 2021 - Levy - Regional Anaesthesia in Patients With DiabetesDocumento9 pagineAnaesthesia - 2021 - Levy - Regional Anaesthesia in Patients With Diabeteseralp cevikkalpNessuna valutazione finora
- Postoperative Ileus Treatment and ManagementDocumento1 paginaPostoperative Ileus Treatment and ManagementdhiyarahadianNessuna valutazione finora
- Dia 2017 2525 AbstractsDocumento134 pagineDia 2017 2525 AbstractsPranav Kumar Prabhakar100% (1)
- Dhatariya Et Al-2012-Diabetic Medicine PDFDocumento14 pagineDhatariya Et Al-2012-Diabetic Medicine PDFkillingeyes177Nessuna valutazione finora
- Diabetic EssayDocumento6 pagineDiabetic Essayreet kaurNessuna valutazione finora
- Diabetes Care After TransplantDocumento16 pagineDiabetes Care After TransplantMazen BarhoushNessuna valutazione finora
- BriatricDocumento5 pagineBriatricmago1961Nessuna valutazione finora
- Pitfalls in Outpatient Diabetes Management and Inpatient Glycemic ControlDocumento7 paginePitfalls in Outpatient Diabetes Management and Inpatient Glycemic ControlUmesh BabuNessuna valutazione finora
- CKD PPKD Weight Reduction 310107Documento3 pagineCKD PPKD Weight Reduction 310107Geoffrey HoNessuna valutazione finora
- Mclain JCDocumento7 pagineMclain JCkenjiNessuna valutazione finora
- Treatment of Patients With Type 1 Diabetes Insulin Pumps or Multiple Injections 2016 Biocybernetics and Biomedical EngineeringDocumento8 pagineTreatment of Patients With Type 1 Diabetes Insulin Pumps or Multiple Injections 2016 Biocybernetics and Biomedical EngineeringJose J.Nessuna valutazione finora
- Nuevas Terapias para La Obesidad - Euro Soc Cardiol 2023Documento18 pagineNuevas Terapias para La Obesidad - Euro Soc Cardiol 2023endobariatryNessuna valutazione finora
- New Technologies and Therapies in The Management of DiabetesDocumento8 pagineNew Technologies and Therapies in The Management of DiabetesArhaMozaNessuna valutazione finora
- 632 Management of Nonalcoholic SteatohepatitisDocumento15 pagine632 Management of Nonalcoholic Steatohepatitispedrogarcia7Nessuna valutazione finora
- Dia 2010 0037Documento8 pagineDia 2010 0037Yigit İskurtNessuna valutazione finora
- Jurnal DindaDocumento6 pagineJurnal Dindachiendo ymNessuna valutazione finora
- Art Cardiologia IIDocumento5 pagineArt Cardiologia IILuis GoncalvesNessuna valutazione finora
- Title of The Research: Diabetes Mellitus By: Abdelrahman Gamal Course Title: Pharmacology Academic Year: Fourth 2019-2020Documento11 pagineTitle of The Research: Diabetes Mellitus By: Abdelrahman Gamal Course Title: Pharmacology Academic Year: Fourth 2019-2020LAZKILLERNessuna valutazione finora
- Hypoglychemia AdultsDocumento32 pagineHypoglychemia AdultsshutekiNessuna valutazione finora
- Chir 1Documento9 pagineChir 1George MogaNessuna valutazione finora
- JurnalDocumento10 pagineJurnalnamartarilia dea najwa kusumaNessuna valutazione finora
- 1123 Insulin ProtocolDocumento7 pagine1123 Insulin ProtocolrosyadNessuna valutazione finora
- Poststroke Hyperglycemia: Natural History and Immediate ManagementDocumento5 paginePoststroke Hyperglycemia: Natural History and Immediate ManagementEsteban Martin Chiotti KaneshimaNessuna valutazione finora
- Insulin TherapyDocumento14 pagineInsulin TherapyElimar Alejandra David GilNessuna valutazione finora
- Laparoscopic Sleeve Gastrectomy: Perioperative Outcomes, Weight Loss and Impact On Type 2 Diabetes Mellitus Over 2 YearsDocumento5 pagineLaparoscopic Sleeve Gastrectomy: Perioperative Outcomes, Weight Loss and Impact On Type 2 Diabetes Mellitus Over 2 YearsYondri Mandaku TasidjawaNessuna valutazione finora
- Cancer GastricoDocumento10 pagineCancer GastricorobertaNessuna valutazione finora
- Continuous Glucose MonitoringDa EverandContinuous Glucose MonitoringWeiping JiaNessuna valutazione finora
- AlbertiDocumento3 pagineAlbertiSuresh GunasekaranNessuna valutazione finora
- TourismDocumento8 pagineTourismSuresh GunasekaranNessuna valutazione finora
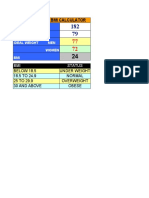
- CALCULATORDocumento1 paginaCALCULATORSuresh GunasekaranNessuna valutazione finora
- WDD Poster ChildrenDocumento1 paginaWDD Poster ChildrenSuresh GunasekaranNessuna valutazione finora