Documenti di Didattica
Documenti di Professioni
Documenti di Cultura
Drug Summary
Caricato da
briancripeDescrizione originale:
Copyright
Formati disponibili
Condividi questo documento
Condividi o incorpora il documento
Hai trovato utile questo documento?
Questo contenuto è inappropriato?
Segnala questo documentoCopyright:
Formati disponibili
Drug Summary
Caricato da
briancripeCopyright:
Formati disponibili
SuperDrugs!
Simon's Short Drug Summary
Acne Gastric Secrection
Goals: ↓ sebum, ↓ inflammation, ↓ bacteria, ↓ keratinisation Goals: ↓ acid secretion, kill Helicobacter pylori
First Line Drugs:
Antiseptic: Benzyl peroxide Proton Pump Inhibitors: -‐prazole eg Omeprazole
• kill proprionibacterium (Gr+) • Irreversibly inhibits H/K ATPase
Keratolytics: Retinoids • A E: rash, headache, diarrhoea (rare)
• Vit A derivatives — kills rapidly-‐dividing cells, ↓ inflammation H2 Receptor Antagonists: ranitidine
If ineffective • Blocks histamine from mast cells → ↓HCl secretion
Antibiotics: **see separate summary** Antacids:
• Doxycycline: oral, topical • Neutralise acid only — Aluminium O H or Mg triscilicate (AE: diarrhoea)
• Clindamycin: topical Anticholinergics: atropine (non-‐specific), pirenzipine (specific)
OCP: if ↑ androgens • Inhibit Ach stimulation of parietal cells
Very Severe Combinations:
Isotretinoin: Triple Therapy: P PI + amoxicillin/cephalosporin + clarithromycin — 2/52
Contra: pregnancy • Abx combination: kill H. pylori + prevent resistance
AE: teratogenic, ↑depression/suicide, C D/UC, alopecia, dry skin [Vit. A toxicity] Quadruple Therapy: Triple Tx + Bismuch Chelate
• Worse for 2-‐4/52, then better by 4-‐8/52 • Bismuth: kills H. pylori, prevents adherence, inhibits enzymes etc
N SAID Use
Lipid-‐lowering drugs Inhibit P G formation (COX inhibitor) → ↓ inhibition of H Cl production
Goal: ↓ serum L DL/VLDL ± ↑ H DL
ECL Cell
First Line
Gastrin
Statins: -‐statin eg atorvastatin (Lipitor)
• H MG CoA Reductase inhibitor — inhibits cholesterol synthesis in liver Cholinergic nerve
Histamine
→ ↑LDL Receptors expressed → ↑ L DL uptake in liver
• A E: ∆GIT, ↑ liver enzymes, rhabdomyolysis
H2 Receptor Anti-‐cholinergics
Resins:
• Sequesters bile salts in gut → ↓ cholesterol absorption & ↑ bile synthesis Antagonists
• A E: G IT – diarrhoea, constipation, ↓ fat-‐soluble vitamin absorption
Fibrates:
• ↓ V LDL production & ↑ Lipoprotein lipase activity → ↑ L DL uptake H2-‐R M3-‐R
• A E: myositis — myglobinuria, A RF
PG Agonists
Others: Adenylate
Misoprostal
• Ezetimibe: ↓ dietary/biliary cholesterol absorption cyclase
↑cAMP
PDE
Asthma Caffeine PG's
Early & late phases AMP
Relievers: ↑PkA & C AM
NSAIDs
Short-‐acting β2 agnoist: salbutamol (Ventolin), terbutaline – inhaled, I V in S.A.
• Bronchodilator: λ=3-‐5hr A E: cardiac effects (overuse – not β2-‐specific)
Long-‐acting β2 agonist: salmeterol, eformoteral — inhaled
K+
• Bronchodilator: λ=12hr
Anticholinergics: ipratropium, tiotropium Parietal Cell
• Muscarinic receptor antagonists – bronchodilatiion, ↓ secretion production
Preventers H+ Cl-‐ K+
Corticosteroids: fluticasone, budesonide, prednisolone
• Anti-‐inflammatory (↓cytokine pdn → ↓ eosinophils & other cells; ↓ P G pdn)
Anti-‐Hypertensives
• Improve β2 effectiveness, but no Sx relief ☺ A AABCDE
Leucotriene receptor antagonist: motelukast, zafirlukast A: ACE inhibitor (captopril, preindopril)
• ↓ chemotaxis, broncho/vasocontriction, permeability and secretions • ↓ Angiotensin 2 effects, ↑ bradykinin = ↓HR, ↑NO = vasodilation
• Adjuvant for mild-‐moderate asthma • A E: hypotension, dry cough, renal impairment
Sodium Cromoglycate: mast cell stabilizer A: AT1 receptor antagonist: candesartan, irbesartan –sartan
• Block ATII binding to AT1 receptor – more specific than ACEi (same M OA)
Allergen / Stimulus • A E: few – dizziness, headache, hyperkalaemia
Th2, monocytes, eosinophil A: α1 antagonist: prazosin
activiation & migration • Blocks postsynaptic α1R (non-‐selective) → prevents N A vasoconstriction
Mast Cells ª A E: orthohTN, nasal congestion, urinary urgency, drowsiness/dizziness
B: β blockers: atenolol (β1 selective), metoprolol (non-‐selective) — ↓HR
cysLT Endothelial • Block β1 (heart) ± β2 (lung/periphery) – ↓HR, ↓force = ↓CO, ↓BP, vasodilation
damage • A E: bradycardia, bronchospasm, dyspnoea, heart block, cold extremities
Histamine, cysLT, C: Ca channel blockers: amlodipine (vascular), verapimil (heart) — ↓ contractility
Chemokines
Spasmogens, P G • ↓ inward Ca in S MC & cardiac cells (L-‐Ca channels)
Airway Airway
Inflammation hyper-‐reactivity D: Diuretics — see separate box
E: Endothelin antagonists: bosentan
Bronchospasm • Blocks endothelin – long-‐acting vasoconstrictor
Bronchoscpasm, • A E: hTN, headache, rash, ↓Hb
β2–antagonists, wheeze, cough
cysLT antagonists
Glucocorticoids
SuperDrugs — Simon Wilson [simon.wilson@uqconnect.edu.au] Page 1 of 5
SuperDrugs! Simon's Short Drug Summary
Antiplatelet Drugs Hypoglycaemics
Prevent platelet aggregation → ↓ coagulation Management of hyperglycaemia, especially in T2DM
Aspirin: C OX inhibitor – also pain relief & antipyretic Sulfonylureas — glibenclamide, glicazide
• Inhibits T XA2 (platelets – aggregation) & P GI2 (endothelia – inhibits) Insulin secreatagogues — ↑ insulin release (upregulate β cells in islets)
→ platelets can't replace T XA2 = nett ↑ inhibition ■ Binds to S UR1 – blocks adjacent K+ channel → Ca influx → insulin release
Epoprosterol: inhibit aggregation, vasodilatation ■ ↓ liver gluconeogenesis
Clopidogrel: blocks A DP receptor → permanent cross-‐linking inhibition ■ Requires functional β cells — not for T1DM or late T2DM (β cells lost)
Glycoprotein I Ia/IIIa antagonists: abciximab, tirofiban Biguanides — metformin
• Inhibit fibrinogen-‐platelet binding – short-‐term Tx
• ↓ hepatic gluconeogensis, ↑ muscle gluconeogensis
• ↑ peripheral glucose uptake,↓ glucose uptake in gut
Anti-‐anginals • A E: lactic acidosis
Goals: ↑ cardiac perfusion, ↓ cardiac metabolic demands • Usable in both T1DM & T2DM
Nitrates Thiazolidinediones — glitazones
• ↓ preload & afterload → ↓ cardiac metabolic demand • ↑ insulin-‐sensitive gene expression → ↑ insulin-‐dependent enzymes
• Redistribute flow to ischaemic areas (collaterals) • A E: retinoedema, cardiac (worsen heart failure)
• ↓ coronary spasm Meglitinides
Glyceryl Trinitrate (GTN): venodilator = ↓ venous return = ↓preload • Short-‐acting insulin secretagogues
• Mode: patch, tablet – rapid tolerance → drug-‐free periods (8-‐12/24) • Also block K cells as sulfonylureas = ↑ insulin production
• A E:postural hypotension, headache • Take with meals
Calcium antagonists (Ca channel blockers) α-‐Glucosidase Inhibitors — metformin
Verapramil/Diltiazem: selective for cardiac/vascular • ↓ glucose breakdown in G IT
• Prevent VG-‐Ca channels opening • A E: flatulence, bloating – not a popular drug
• A E: constipation, headache
Sulfonylurea
β adrenoreceptor antagonists
• ↓HR & ↓ metabolic demand
Propranolol, metoprolol, atenolol
Contra: asthma, diabetes + SUR1
• ↓ chronotropic & ↓ inotropic states = ↑ filling time for coronary vessels Ca+ K+
Anticoagulants +
β
Cell
Prevent
the
formation
of
thrombi (Pancreas)
Heparin
—
I V
Insulin
•
Short-‐term
(60-‐90
min
onset),
easily
reversed
(IV
protein
to
neutralise
acid)
•
Activates
antithrombin
3
(AT
I II)
–
inhibits
factors
I Ia
(thrombin)
&
Xa Anti-‐neoplastics
*
Prevents
fibrinogen→fibrin
by
thrombin Kill
tumour
cells
and/or
halt
tumour
growth
•
A E:
haemorrhage
(especially
wounds),
osteoporosis
LMWH:
longer
lasting,
more
predictable
(affect
Xa
>
I Ia)
–
enoxaparin,
dalteparin Cytotoxics
Hirudin/Bivalirudin:
direct
thrombin
inhibitors
–
superior
to
Heparin,
I V
only Alkylating
agents:
cyclophosphamide
—
N S
Avugatram:
orally
active
X Ia
inhibitor
–
future
direction...
•
Cross-‐links
D NA
strands
–
prevents
replication
•
Metabolised
to
phosphoramide
mustard
(active)
&
acrolein
(AE's)
Warfarin
—
oral
•
Caution
in
renal
patients
•
Prolonged
Tx
(2-‐3/7
onset
—
↑
prothrombin
stores)
•
A E:
haemorrhagic
cystitis
(accumulate
in
bladder),
alopecia,
anorexia
•
Prevents
Vitamin
K
reductase
action
Anthracyclines:
doxorubicin
—
S-‐phase
–
Essential
for
factors
2,
7,
9
and
10
and
proteins
C
&
S
•
Affects
topoisomerase
I I
function
–
prevent
repair
of
D NA
strand
breaks
•
A E:
haemorrhage,
teratogenic
(eye,
limb,
C NS
defects)
•
Caution:
liver
impaired,
<
4
yo,
radiotherapy
•
Reduced
effectiveness
if
↑VitK
intake
(leafy
vegetables)
Antimetabolites:
methotrexate
(G1–S
phase)
•
Overdose:
VitK
administration
•
Inhibits
Dihydrofolate
reductase
(DHFR)
=
↓
folate-‐dependent
D NA
synth
•
Caution:
renal/liver
impairment,
radiotherapy,
P UD
Thrombylytics
/
Fibrinolytics
•
A E:
N&V,
anorexia,
alopecia,
myelosupression
Catalyse
fibrin
breakdown
Platinum:
cysplatin
—
N S
Convert
plasminogen→plasmin
•
Free
radical
formation
inside
cells
→
D NA
damage,
apoptosis
Digests
fibrin,
fibrinogen,
and
factors
I I,
V
and
V II
•
Caution:
hearing
impairment,
renal
impairment
–
ototoxic
&
nephrotoxic
Streptokinase
—
I V Vinca
Alkaloids:
antitubulins
&
antimitotics
—
vincristine,
docetaxel
(M
phase)
•
Synthesised
by
haemolytic
streptococci
—
will
develop
Ab's
if
repeated
<
6/12
•
Inhibits
microtubule
formation
→
mitotic
arrest
•
First-‐line
in
acute
M I
•
Contra:
radiotherapy
•
Less
selective
that
tPA
—
activates
bound
and
circulating
plasminogen
•
A E:
alopecia,
abdo
pain,
constipation,
fatigue,
fever,
neurotoxic
Non-‐cytotoxic
Tissue
Plasminogen
Activator
(tPA)
—
I V
Antibodies:
trastuzamab
•
Natural
plasminogen
activator
from
endothelial
cells
–
recombinant
•
Binds
H ER2
receptor
(breast
ca.
–
growth
stimulator)
–
blocks
cascade
•
Selective
for
bound
plasminogen
at
low
concentrations
•
Cell
targeted
by
immune
system
&
receptor
endocytosed
(↓
expression)
-‐
But
need
high
concentration
to
dissolve
within
1hr
of
M I
→
not
selective Tyrosine
Kinase
Inhibitors:
imatinib
(inhibit
B CR:ABL
T K
in
Philadelphia
chr)
•
Decreases
intercellular
signalling
Gout
•
Not
curative
–
only
decreases
growth
Prevent
&
reduce
urate
crystal
formation Hormonal
GOUT: Selective
Oestrogen
Receptor
Modulators
(SERMs):
tamoxifen
Allopurinol:
xanthine
oxidase
inhibitor
–
lowers
urate
production
from
xanthine
•
Competes
with
oestrogen
at
receptor
sites
in
breast
cancer
–
↓
growth
•
Used
to
prophylactic
&
treatment
of
hyperuricaemia
(high-‐cell
turnover)
Colchicine:
gout
and
anti-‐inflammatory
•
Inhibits
neutrophil
migration,
chemotaxis,
adhesion
&
phagocytosis
SuperDrugs — Simon Wilson [simon.wilson@uqconnect.edu.au] Page 2 of 5
SuperDrugs! Simon's Short Drug Summary
Fertility Drugs Analgesics, Antipyretics & Anti-‐inflammatories
Increase ovulation Pain relief & fever reduction
Oestrogen Antagonist: clomiphene citrate Non-‐Opoids
Indic: sub-‐fertility due to anovulation, unexplained infertility Aspirin: N SAID – mainly C OX1 selective
MOA: binds oestrogen receptors in hypthalamus-‐pituitary axis = ↓ feedback • Has anti-‐platelet effect (COX1)
• Causes prolonged & increased F SH production→ ↑ follicle development time Ibuprofen: non-‐selective N SAID – reversible
• Used for 2/52 post-‐menstruation – withdrawal = ovulation Paracetamol: not an N SAID — C OX3 inhibitor?
Caution: ↑ risk of multiple births • Primarily analgesic & antipyretic (minimal inflammatory role)
Most conceive within 1 year • Antipyretic: ↓ hypothalamus P G production — mild P G decrease overall
Celecoxib: C OX2-‐selective N SAID
Contraceptives • Use: OA, R A, dysmenorrhea, familial adenomatous polyposis
Prevent implantation • Still has G IT A E's despite minimal C OX1 effect
Combined Oral Contraceptive NSAIDs:
• All analgesic, antipyretic & anti-‐inflammatory agents
• Combines Oestrogen & Progesterone
• ↓ G FR — caution in renal patients
-‐ P: ↓GnRH = ↓LH/FSH → scanty/thick cervical mucous, ↓ follicle maturation
• Most non-‐selective for C OX1 (AE) & C OX2 (treatment)
-‐ E: prevent L H/FSH surge = Ø ovulation, inhibits implantation
• Monophasic (same dose for 21/7) or triphasic (alters throughout cycle) Opoids
• More effective than P-‐only pills in < 40 yo Opioids: opioid-‐like effects, regardless of structure
• ↓ risk endometrial, ovarian & colorectal cancer Opiate: structurally similar to morphine & similar action
• ↑ risk breast, cervical & liver cancer, C VD, depression Act through 3 receptors: μ, δ, κ — G-‐protein coupled receptors
• ↓ iron loss in mensrual blood • Opioids activate µ receptors
• ↑ bone mineral density • δ: peripheral pain relief
Intrauterine Contraceptive Device (IUD): • κ: spinal analgesia
• Plastic or copper insert — lasts up to 10 years
Codeine: activates C NS & P NS opioid receptors
• Releases progesterone (Mirena), interrupts implantation
• Analgesic, respiratory depression, sedation, constipation (↓ motility)
• Metabolised to morphine in body (6-‐10% lack necessary enzyme)
Osteoprosis • ↓ N T transmission & neuronal excitability – pre-‐ & post-‐synaptically
Prevent dysregulated bone resorption • Leads to dependence & substance abuse
Bisphosphonates: pamidronate (Op, Pagets, malig.), alendronate (Op, Paget's) • Good oral availability
MOA: Bind to bone – inhibit O C activity, trigger O C apoptosis Morphine:
• Given I V every 3-‐12/12 — poor lipid solubility = ↓ bioavailability • No anti-‐diarrhoeal effect, despite slowing G IT motility
• λ up to 10 years — bind in areas of good blood supply • Tolerance develops quickly (req dose adjustment) – dependence & abuse
AE: G IT upset, osteonecrosis of jaw (rare) • I V: poor oral uptake
Stontium Ranelate Methadone:
• Good oral uptake, long λ & ↓ effects
MOA: poorly understood – inhibit O C & stimulate O B?
• Also blocks N MDA (glutamate) receptors — ?MOA for ➘ dependence
Orally active, taken mane
Oestrogen
Antidepressants
MOA: ↓IL-‐6 → O C inhibition Alleviate depressed mood disorders
• Combine with progesterone if pt has not had hysterectomy
Calcitriol Tricyclic Antidepressants (TCA) — doxepin
MOA: ↑ G IT Ca uptake, ↑OB activity Inhibit N A & 5HT reuptake into presynaptic C NS neurons
• Risk of hypercalcaemia • ↑ N T in synaptic cleft → ↑ excitation
No effects on dopamine
Calcitonin
AE: cardiac & respiratory depression
MOA: unsure — no evidence for use, but last resort for unresponsive pts
Selective Noradrenalin Reuptake Inhibitors (SNaRI) — venlafaxine (Efexor)
Similar to TCAs with ↓ A Es & no O/D
Benzodiazepines
Slow-‐release daily tablet
Anxiolytic & hypnotic
Selective Serotonin Reuptake Inhibitors (SSRI) — fluoxitine (Prozac)
Inhibitory effects on G ABA throughout C NS Inhibits 5HT reuptake only — minimal effects on N A and D A
• G ABA-‐a: ligand-‐gated Cl channels — opened = hyperpolarise (↓excitation) Safer than TCAs (wide therapeutic window) — O/D = serotonin syndrome
Anxiolytic, sedative, hypnotic, muscle relaxant, anti-‐epileptic
Monoamine Oxidase Inhibitors (MAOI) — phenelzine
AE: respiratory depression, paradoxical disinhibition, psychomotor retardation,
tolerance, depression, emotional blunting Inhibit M AO – breaks down N Ts once reuptaken → more N T available
Contra: alcohol use, teratogenic (class D) Used only if other antidepressants do not have desired affects
Reversed by flumazenil – competitively binds to benzo site • React with tyramine (cheese reaction) → H TN, headache, intracranial bleeds
Atypical Antidepressants — mirtazapine
Dazepam: 24-‐48 hrs
Midazolam: 12-‐18 hrs Do not have traditional antidepressant M OA
Temazepam: < 6 hrs • α-‐adrenoceptor inhibition: blocks inhibition of 5HT/NA release
• 5HT2/3 receptor inhibition: ↑ 5HT1 action = antidepressant w/o N&V!
AE: dry mouth, sedation, ↑wt
SuperDrugs — Simon Wilson [simon.wilson@uqconnect.edu.au] Page 3 of 5
SuperDrugs! Simon's Short Drug Summary
Antibiotics Antivirals
Prevent
&
reduce
urate
crystal
formation
Bacterial
cell
wall
synthesis
inhibitors
–
cidal Nucleoside
Analogues:
guanine
analogues,
inhibit
D NA
polymerase
β-‐lactams:
binds
penicillin
binding
peptides
(PBPs)
•
acyclovir
(herpes),
caniciclovir
(CMV)
•
Inhibits
translinking
of
peptidoglycan
layer
(transpeptidase
inhibition) Nucleoside
Analogue
Reverse
Transcriptase
Inhibitors:
compete
for
R T's
-‐
Penicillins:
amoxicillin
•
zidovudine
-‐
Cepahlosporins:
cephalexin Non-‐nucleoside
Reverse
Transcriptase
Inhibitors:
alters
R T
activity
Glycopeptides:
vancomycin
—
block
transpeptidase
&
peptidoglycan
synthase
•
nevirapine
Protein
Synthesis
Inhibitors HIV
Protease
Inhibitors:
prevents
precursor
cleavage
into
proteins
–
↓mutation
Macrolides:
erythromycin,
clarithromycin,
roxithromycin
[50s]
-‐static
•
saquinovir
Aminoglycasides:
gentamicin
[30s]
-‐cidal Amantadine
/
Rimantadine:
inhibits
viral
uncoating
–
Influenza
A
Lincosamides:
clindamycin
[50s]
-‐static Neuroaminidase
inhibitors:
inhibits
viral
shedding
Tetracyclines:
doxycycline
[30s]
-‐static
•
zanimivir,
oseltamivir
–
influenza
A
&
B
Chloramphenicol:
[50s]
–static Interferons:
boost
host
immune
response
–
recombinant
I FNa's
Nucleic
Acid
Interferants
Rifamycin:
rifampicin
—
inhibits
bacterial
R NA
polymerase
(TB,
M RSA)
-‐static Antifungals
Quinolones:
ciprofloxacin
—
D NA
gyrase
(Gr–)
&
topoisomerase
(Gr+)
-‐cidal
Nitromidazole:
metronidazole
—
form
free
radicals
when
metabolised
-‐cidal Polyene
Antifungals:
binds
ergosterol
in
wall
–
forms
porin
[static/cidal]
Antimetabolites
/
Folate
Inhibitors
•
amphotericin
B
Linezolid:
inhibits
50s
subunit
–
M RSA,
V RE Azole
Antifungals:
block
ergosterol
production
(lanosterol
12a-‐demethylase)
Clavulanic
acid:
binds
to
β-‐lactamase
→
↑β
lactam
effect
(not
an
antibiotic)
•
flucanozole,
ketocanozole
[static]
Allyamines:
block
ergosterol
synthesis
(squaline
epoxidase)
[cidal]
Corticosteroids
•
terbinafine
Hormones
produced
in
adrenal
cortex Echinocandins:
inhibt
B
glucan
synthesis
(cell
wall
maintenance)
[cidal]
Glucocorticoids
—
cortisol
(also
has
some
action
against
mineralocorticoids)
•
casofungin
MOA:
bind
to
cytoplasmic
glucocorticoid
receptor
(GR)
→
D NA
binding
site DNA
Synthase
Inhibitors:
inhibit
D NA
&
R NA
synthesis
–
substrate
analog
•
Transactivation:
activation
of
gene
•
flucytosine
[cidal]
•
Transrepression:
repress
cyto/chemokine,
adhesion
molecule
&
inflam
proteins Antimitotic:
binds
tubulin
–
inhibits
cell
division
[static]
Low
dose:
hormone
replacement,
adrenal
insufficiency
•
Griseofulvin
High
dose:
immunosupression,
anti-‐inflamm,
chemo-‐induced
nausea
relief
(↑AE) Anti-‐malarial
Agents
AE:
poor
healing,
infection,
dyspepsia,
oedema,
iatrogenic
Cushing's,
acute
Prevent
&
kill
parasite
(Plasmodium
falciparum,
malariae,
vivax,
ovale)
adrenal
insufficiency
(on
withdrawal),
osteoporosis
(↑OC
activity)
Directions:
take
with
meals,
don't
stop
suddenly,
see
Dr
if
infection
begins Schizonticides:
Prednisolone:
Quinine:
kill
parasite
within
R BC
–
therapeutic
(PF,
P M)
/
suppress
(PV,PO)
•
Use:
Anti-‐inflam
(asthma),
auto-‐immune
disease
&
croup
•
M OA:
Inhibits
haem
polymerase
→
haem
aggregates
in
parasite
(cytotoxic)
•
↓
capillary
dilation,
oedema,
fibrin
deposition,
leukocyte
migration,
scarring
•
A E:
cinoconism
(flushed
sweaty
skin,
blurred
vision,
tinnitus,
↓hearing,
•
A E:
osteoporosis,
poor
healing,
immune
suppression,
↓
growth
confusion,
abdo
pain,
photosensitivity,
N
&
V
&
D.
Beclomethasone: Cholorquine:
kills
parasite
–
prophylactic
&
therapeutic
•
Use:
asthma
(prophylacticly)
•
M OA:
as
quinine
•
Poor
absorption
–
inhaled
for
airway
inflammation
•
Resistance
developed
–
↓
uptake
•
A E:
osteoporosis,
poor
healing,
immune
suppression,
↓growth,
candidiasis Mefloquine:
kills
parasite
–
prophylactic
&
therapeutic
•
M OA:
unknown
–
?
toxic
complexes
with
heme
→
parasite
death
Inflammatory
Bowel
Disease
•
Used
for
chloroquine-‐resistant
Plasmodium
Radical
Cure
Doxycycline:
tetracycline
antibicrobial
–
inhibits
30s
ribosome
&
protein
synth
5-‐Aminosalicylates
—
mesalamine
•
A E:
photosensitivity,
candidiasis,
oesophagitis
GIT-‐specific
anti-‐inflammatory
–
C OX
&
5-‐lipoxygenase
inhibitors
=
↓PG,
↓LT Artemisin:
produces
reactive
oxygen
radical
during
haem
breakdown
•
May
↓
chemotaxis
(Mϕ
&
Nϕ),
I NFγ,
T NFα
•
Used
in
conjunction
with
mefloquine
Bound
to
sulfapyridine
–
broken
in
gut
=
maximal
effect
there Pyrimethimine
/
Sulfodoxine:
Fansidar
•
Sulfapyridine
causes
A E:
fever,
malaise,
N&V,
headache,
↓folate
•
D HFR
inhibitor
+
sulfonamide
(also
D HFR
inhibitor)
–
selective
for
Plasmodium
Contra:
aspirin
allergy
(similar
structure) Malarone
–
atovaquone
+
proguanil
Corticosteroids:
•
Parasite
mitochondrial
E TC
inhibitor/pyrimidine
synthesis
inhibitor
↓LT,
↓PG,
↓cytokines,
↓adhesions,
↓IgE-‐dependent
histamine
release
+
Plasmodium
D HFR
inhibitor
Oral
use
in
exacerbations
(UC
>
C D)
—
remission,
not
maintenance
Prevention
Methods
Immunosuppressants: Gamete
destruction:
Primaquine,
proguanil,
artemisinin,
pyrimethimine
Azothioprine,
6-‐Mercaptopurine:
thioguanine
derivatives
–
inhibit
purine
synth
•
Slow
onset
(3-‐6/12)
–
maintenance
Anti-‐emetics
&
Emetics
•
Caution:
allopurinol
(xanthine
oxidase
required
to
break
down
6-‐M.) Prevent
&
induce
vomiting
Methotrexate:
folate
analogue
•
Cytotoxic,
immunosupressive
&
anti-‐inflammatory
roles Anti-‐emetics
—
antagonise
Ach,
histamine,
5HT
and
dopamine
Cyclosporin:
calcineurin
inhibitor
(↓IL-‐2) H1
Antagnoists:
promethazine
—
motion
sickness,
morning
sickness
•
↓
T
cell
response
in
severe
U C
—
remission,
not
maintenance
•
A E:
drowsiness,
sedation
•
A E:
nephrotoxic,
H TN,
hyperlipidaemia,
gum
hyperplasia,
induce
diabetes Muscarinic
receptor
antagonists:
hyoscine
—
morning
sickness
•
A E:
drowsiness,
dry
mouth,
blurred
vision
Anti-‐T NFα
Agents: D2
Receptor
antagonists:
metoclopramide,
prochlorperizine
inflixamib:
anti-‐T NFα
antibody
–
I V
infusion,
repeated
for
maintenance
•
Use:
radiation-‐induced,
gastroenteritis,
cytotoxic-‐induced,
anaesthesia
•
S E:
sedation,
hypotension
5HT
Receptor
antagonists:
ondansetron
—
cancer,
anaethetic,
radiation
•
S E:
headache,
G IT
uptset
Emetics
Ipecacuanha:
induce
if
toxic
substance
swallowed
&
patient
is
conscious
SuperDrugs — Simon Wilson [simon.wilson@uqconnect.edu.au] Page 4 of 5
SuperDrugs! Simon's Short Drug Summary
Anti-‐arrhythmics Heart Failure
Reduce cardiac arrythmias — many are proarrhythmic too! ↓ contractility & ↓CO
Class 1 — Na Channel Blockers: ↓ Na influx = slow depolarisation Compensations: ↑ preload, hypertrophy, ↑ hormones (NA, AT3, vasopressin)
1a: Intermediate dissociation – quinidine, procainamide Tx: diuretic, +ve inotrope (digoxin), vasodilator (ACEi), β-‐blocker
• Use: A F, ventricular arrhythmias, paroxysmal S VT → improve contractility & decrease workload of heart
• Lengthens phase 0 = lengthens A P Diuretics: ↓ preload
• Anti-‐cholinergic – ↑ AV conduction delay Rapidly decrease dyspnoea & peripheral oedema
• Also blocks some K efflux → longer repolarisation Can cause arrhythmias – induce ↓K, ↑urate, over-‐diuresis
• A E: cinchonism (arrhythmia, cardiotoxic, pain, rashes, hearing loss, blindness) Loop diuretics: frusemide (Lasix) – rapid onset, short duration
1b: Fast dissociation – lignocaine • M OA: block Na/K/2Cl channel in thick ascending LoH
• Use: during/after M I, V T, V Fib, V Flutter, re-‐enterant ventricular arrhythmia K Loss: Blocking Na resorption → ↑Na
Thiazide: hydrochlorothiazide
• Selective for damaged cells (↑RMP) – ↑ refractive ⌚, ↑ depolarisation, ↓AP • M OA: blocks Na/Cl channel in D CT to D CT → ↑ENaC Na/K exchange
1c: Slow dissociation – flecainide • Monitor electrolytes closely = ↑K excretion
• Use: paroxysmal S VT, A F, V T • Combine with loop diuretic if severe H F — less effective if ↓GFR
• Lengthens depolarisation, no change to A P – non-‐selective Amiloride:
Class 2 — β-‐adrenoreceptor Antagonists • M OA: blocks E NaC in D CT & CCT — weakly diuretic (combine with others)
• β1-‐selective: metoprolol, atenolol Spironolactone:
• Non-‐selective β: propranolol • M OA: blocks aldosterone from ↑Na/K pump → ↓Na resorption
• Non-‐selective β + α1: labetalol • Improves survival at sub-‐therapeutic levels – ↓ heart fibrosis
MOA: prevent N A-‐induced ↑influx of Na & Ca • A E: gynaecomastia, hirsuitism
• ↓ phase 4 in pacemaker cells = ↑ A P
Contra: asthma, diabetes Positive Inotropes
Use: S VTs — targeted at S A & AV nodes
Digoxin: (see anti-‐arrhythmics) — last-‐resort drug for end-‐stage H F
Class 3 — K Channel Blockers
• ↑ contractility, ↑ urine output, ↓SNS & renin effects
MOA: prolong phase 3 – block efflux & repolarisation → ↑AP • A E: arrhythmia, digoxin toxicoses (↑λ, anorexia, N&V), AV block
Use: W PW, A F, V T Calcium sensitisers: levosimendan
Amiodarone: ↓ re-‐entry and automaticity, ↑AP — most effective drug • M OA: ↑Ca binding to contractile proteins (not in emergency situations)
• A E: paraesthesia, h/a, constipation, pigmentation, corneal deposit, Dobutamine, Dopamine: emergency use only (↓λ)
photosensitivity, pulmonary fibrosis • M OA: similar to N A, but less ↑HR
D-‐Sotalol: L-‐isomer of β-‐blocker Vasodilators: ↓ afterload, ↑CO
• Caution: can increase risk of arrhythmia with old infarcts
ACEi: captopril
Class 4 — Ca Entry / Channel Blockers
• M OA: decreases hypertrophy, hyperplasia, vasoconstriction, fibrosis,
Verapamil, diltiazem, (nifedipine) Contra: β-‐blocker – heart block aldosterone release, oxidative stress to endithelial cells
MOA: blocks inwards Ca channels
• A E: ↑ bradykinin = dry cough
• ↓ impulse conduction: AV node & damaged tissue
Angiotensin I I Receptor Antagonistsb: candesartan, irbesartan
• Shortens phase 2 (plateau) = ↓AP
• M OA: AT1R antagonists — ATiii can then target AT2R
• Negative inotropic
• A E: limited — no cough
Use: S VT, A F, +ve inotropic states β-‐Adrenoreceptor Antagonists
Class 5 — Others
Carvedilol (non-‐selective), metoprolol (selective)
Digoxin: + inotrope
• ↓HR, ↓contractility, ↓renin release (↓AT2)
MOA: Na/K channel blocker = ↑ intracellular Na = ↓Ca efflux
• Symptomatic improvements, ↑exercise tolerance, ↑LV function, ↑survival
• Increases vagal tone on AV node = ↓ chance of A F passing to ventricles
Use: A Fib, A Flutter — not for ventricular arrhythmias
Contraindicated Drugs
Adenoside: rapid transient AV node blocker
Ca Channel Blockers, α-‐adrenoreceptor blockers, nitrates (tolerance)
MOA: Hyperpolarisation: inhibit adenylyl cyclase → ↓cAMP → ↑K efflux
Use: acute S VT (AF)
1
Antibiotics
Prevent & reduce urate crystal formation
0 mV
2 Class 1a Bacterial cell wall synthesis inhibitors – cidal
β-‐lactams: binds penicillin binding peptides (PBPs)
• Inhibits translinking of peptidoglycan layer (transpeptidase inhibition)
-‐ Penicillins: amoxicillin
-‐ Cepahlosporins: cephalexin
3 Class 1b
-‐50 mV Glycopeptides: vancomycin — block transpeptidase & peptidoglycan synthase
0
Protein Synthesis Inhibitors
Macrolides: erythromycin, clarithromycin, roxithromycin [50s] -‐static
Threshold Aminoglycasides: gentamicin [30s] -‐cidal
Class 1c Lincosamides: clindamycin [50s] -‐static
4 4 Tetracyclines: doxycycline [30s] -‐static
-‐100 mV Chloramphenicol: [50s] –static
Nucleic Acid Interferants
Rifamycin: rifampicin — inhibits bacterial R NA polymerase (TB, M RSA) -‐static
Quinolones: ciprofloxacin — D NA gyrase (Gr–) & topoisomerase (Gr+) -‐cidal
Nitromidazole: metronidazole — form free radicals when metabolised -‐cidal
Antimetabolites / Folate Inhibitors
Linezolid: inhibits 50s subunit – M RSA, V RE
Clavulanic acid: binds to β-‐lactamase → ↑β lactam effect (not an antibiotic)
SuperDrugs — Simon Wilson [simon.wilson@uqconnect.edu.au] Page 5 of 5
Potrebbero piacerti anche
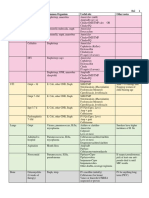
- Lile Bai 1: Area/Site Common Organism Useful Abx Other NotesDocumento3 pagineLile Bai 1: Area/Site Common Organism Useful Abx Other NotesNicole BerryNessuna valutazione finora
- The Principles of Antibiotic Therapy: S. Aureus Streptococcus PneumoniaeDocumento16 pagineThe Principles of Antibiotic Therapy: S. Aureus Streptococcus PneumoniaeDianne Chua100% (7)
- Pharmacology Drug Chart: Drug Name Receptor Therapeutic Uses Adverse EffectsDocumento18 paginePharmacology Drug Chart: Drug Name Receptor Therapeutic Uses Adverse EffectsPadmavathy Naidu Chokkapu100% (2)
- Pharmacology Mnemonics (Part 01) by M IhtishamDocumento32 paginePharmacology Mnemonics (Part 01) by M Ihtishammuhammad ihtisham ul hassan100% (1)
- A.1. Community-Acquired: Use Antibiotics JudiciouslyDocumento33 pagineA.1. Community-Acquired: Use Antibiotics JudiciouslymaxgroovesNessuna valutazione finora
- Inhibit Clasification Antibiotics: (Broad Spectrum) (Narrow Spectrum)Documento1 paginaInhibit Clasification Antibiotics: (Broad Spectrum) (Narrow Spectrum)SY WongNessuna valutazione finora
- AB ClassesDocumento4 pagineAB Classesrayooona88100% (2)
- Review Handouts For Medical Pharmacology PDFDocumento21 pagineReview Handouts For Medical Pharmacology PDFAndres F. TorresNessuna valutazione finora
- Antibiotic TableDocumento7 pagineAntibiotic TablenkuligowskiNessuna valutazione finora
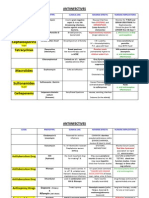
- AntimicrobialsDocumento1 paginaAntimicrobialsRomaine Barrett100% (1)
- Pharmacology Complete Drug TableDocumento6 paginePharmacology Complete Drug Tableninja-2001100% (4)
- Antibiotic Study Cheat Sheet October 2018Documento1 paginaAntibiotic Study Cheat Sheet October 2018Nourhan100% (3)
- Infectious Diseases IDocumento7 pagineInfectious Diseases ITiff VoNessuna valutazione finora
- Antibiotics Handout ReferenceDocumento3 pagineAntibiotics Handout Referencebl9nkverseNessuna valutazione finora
- Pharm Drug ListDocumento17 paginePharm Drug Listanon_523534678Nessuna valutazione finora
- Respiratory System: Antiasthmatic Drugs Cardiac GlycosidesDocumento4 pagineRespiratory System: Antiasthmatic Drugs Cardiac GlycosidesNurse HoomanNessuna valutazione finora
- Antibiotics Quick ReviewDocumento5 pagineAntibiotics Quick Reviewpranjl100% (5)
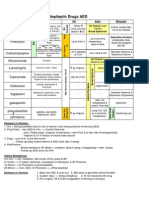
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDocumento1 paginaAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88Nessuna valutazione finora
- Beta Lactam AntibioticsDocumento1 paginaBeta Lactam AntibioticsCourtney TownsendNessuna valutazione finora
- Drug Interactions 2 Paper PDFDocumento2 pagineDrug Interactions 2 Paper PDFAzima AbdelrhamanNessuna valutazione finora
- Pharmacology MnemonicsDocumento19 paginePharmacology MnemonicsAl-nazer Azer Al100% (5)
- Antihypertensive AgentsDocumento2 pagineAntihypertensive Agentskryscae nacarNessuna valutazione finora
- Total Pharmacy Notes TPN For EEDocumento1.601 pagineTotal Pharmacy Notes TPN For EEClaire Cura100% (2)
- Antibiotics Chart 2Documento10 pagineAntibiotics Chart 2Vee MendNessuna valutazione finora
- Antibiotics Summary - Flattened PDFDocumento3 pagineAntibiotics Summary - Flattened PDFmicheal1960100% (6)
- Induction Agents MOA Onset, Duration Special Uses / Notes PropofolDocumento3 pagineInduction Agents MOA Onset, Duration Special Uses / Notes PropofolpaveethrahNessuna valutazione finora
- DRUG of CHOICE - InfectiousDocumento1 paginaDRUG of CHOICE - InfectiousJoseph De JoyaNessuna valutazione finora
- AntibioticsDocumento11 pagineAntibioticsSeshu Kelam100% (2)
- Antiinfectives Drug TableDocumento5 pagineAntiinfectives Drug Tablecdp1587100% (3)
- Antibiotics Cheat SheetDocumento2 pagineAntibiotics Cheat SheetAlejandro Rodas Salinas100% (1)
- Year 2 Drug ListDocumento8 pagineYear 2 Drug ListRay100% (1)
- Antibiotics ChartDocumento10 pagineAntibiotics Chartadom09Nessuna valutazione finora
- Pharmacology SummaryDocumento16 paginePharmacology Summaryshenric16Nessuna valutazione finora
- Antibiotics - Pathogen ChartDocumento3 pagineAntibiotics - Pathogen ChartYanling LiNessuna valutazione finora
- Class Medication MOA Side Effects: Intranasal SteroidsDocumento2 pagineClass Medication MOA Side Effects: Intranasal SteroidsChron MedNessuna valutazione finora
- AntibioticsDocumento6 pagineAntibioticsCyrus100% (1)
- AntibioticsDocumento9 pagineAntibioticsprince1500100% (1)
- Antibiotics 101Documento49 pagineAntibiotics 101Tony VoNessuna valutazione finora
- Vancomycin Pharmacology Indications, Mechanism, and Side Effects! PDFDocumento1 paginaVancomycin Pharmacology Indications, Mechanism, and Side Effects! PDFFrancis PasayNessuna valutazione finora
- AntibioticsDocumento6 pagineAntibioticsOccamsRazor100% (1)
- Pharma ChartsDocumento33 paginePharma ChartsNooreen Hussain100% (1)
- Mnemonics For AntibioticsDocumento10 pagineMnemonics For AntibioticsShane AllenNessuna valutazione finora
- Classification of AntibioticsDocumento5 pagineClassification of AntibioticsdenaNessuna valutazione finora
- Top 300 Drugs Pocket Reference Guide (2021 Edition)Da EverandTop 300 Drugs Pocket Reference Guide (2021 Edition)Valutazione: 5 su 5 stelle5/5 (1)
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesDa EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesValutazione: 4 su 5 stelle4/5 (2)
- 8 ToxicologyDocumento5 pagine8 ToxicologyMd Sakil AminNessuna valutazione finora
- Class 5 Cholinergic SystemDocumento25 pagineClass 5 Cholinergic SystemDr.U.P.Rathnakar.MD.DIH.PGDHMNessuna valutazione finora
- Peptic UlcerDocumento60 paginePeptic Ulcerdiwakar4123sawNessuna valutazione finora
- Antidotes and The Clinical Applications Antidote: An Antidote Is A Substance Which Can Counteract A Form ofDocumento2 pagineAntidotes and The Clinical Applications Antidote: An Antidote Is A Substance Which Can Counteract A Form ofManohar Chowdary KovvuriNessuna valutazione finora
- AutacoidsDocumento12 pagineAutacoidsRamiz IsrafNessuna valutazione finora
- Pharma ReviewerDocumento74 paginePharma ReviewerSamantha DiegoNessuna valutazione finora
- 4 AutacoidsDocumento9 pagine4 AutacoidsAli EllaffiNessuna valutazione finora
- Emergency DrugsDocumento17 pagineEmergency Drugsapi-3853350100% (12)
- P2 Pharma NotesDocumento3 pagineP2 Pharma NotesDindin GalgoNessuna valutazione finora
- Cardiovascular DiseasesDocumento8 pagineCardiovascular DiseasesRebecca MarshallNessuna valutazione finora
- Anti Hypertensive AgentsDocumento38 pagineAnti Hypertensive Agentskrishkodal0020Nessuna valutazione finora
- Anti HistaminesDocumento5 pagineAnti HistaminesAnkit PandeyNessuna valutazione finora
- Pharm Study NotesDocumento6 paginePharm Study Notesapi-663458841Nessuna valutazione finora
- Drug Summary Chart 1Documento16 pagineDrug Summary Chart 1Maya U100% (1)
- Chapter Seven The Behavior of Proteins: Enzymes, Mechanisms, and ControlDocumento40 pagineChapter Seven The Behavior of Proteins: Enzymes, Mechanisms, and ControlSheila GarciaNessuna valutazione finora
- 20312e00 Guidelines For Chemical Treatments of PipelinesDocumento68 pagine20312e00 Guidelines For Chemical Treatments of Pipelinesamra_41100% (4)
- Shivansh Pande Clinical Pharmacist Apollo Hospitals, Jubilee Hills, HyderabadDocumento12 pagineShivansh Pande Clinical Pharmacist Apollo Hospitals, Jubilee Hills, HyderabadshivanshpandeNessuna valutazione finora
- DocumentDocumento21 pagineDocumentArturo Macaranas100% (1)
- Martins 2016Documento10 pagineMartins 2016rohmeNessuna valutazione finora
- Bluff EnzymesDocumento51 pagineBluff EnzymesJay Andrea Vea Dayuday-IsraelNessuna valutazione finora
- Medical Biochemistry: Enzymes: Mr. Genaro F. Alderite JR, MsermDocumento58 pagineMedical Biochemistry: Enzymes: Mr. Genaro F. Alderite JR, MsermNash DeniegaNessuna valutazione finora
- Lesson Plan March 29, 2019 Biochemistry Chapter 5 Topic: Enzymes Pp. 43-47Documento3 pagineLesson Plan March 29, 2019 Biochemistry Chapter 5 Topic: Enzymes Pp. 43-47enilegnavemartinezNessuna valutazione finora
- DigoxinDocumento6 pagineDigoxinSEIYADU IBRAHIM KNessuna valutazione finora
- Primary & Secondary MetabolitesDocumento4 paginePrimary & Secondary MetabolitesChandra ReddyNessuna valutazione finora
- International Biology Olympiad - Hong Kong Contest 2018 - 2018Documento70 pagineInternational Biology Olympiad - Hong Kong Contest 2018 - 2018Ngọc CaiNessuna valutazione finora
- Biochemistry of Enzymes & Clinical Enzymology: By: Tesfahun MollaDocumento156 pagineBiochemistry of Enzymes & Clinical Enzymology: By: Tesfahun MollaAddis MémñøňNessuna valutazione finora
- Mok QuestionDocumento28 pagineMok QuestionikaNessuna valutazione finora
- Sultrine Sultrine: Sulfadiazine Sulfamerazine Sulfamethazine Sulfadiazine Sulfamerazine SulfamethazineDocumento3 pagineSultrine Sultrine: Sulfadiazine Sulfamerazine Sulfamethazine Sulfadiazine Sulfamerazine SulfamethazineFaith de Leon ♥100% (1)
- MCQ Sample Test Paper-Dotes PharmaDocumento7 pagineMCQ Sample Test Paper-Dotes PharmaDominus TestimoniumNessuna valutazione finora
- ActiguardDocumento2 pagineActiguardAlex K.Nessuna valutazione finora
- Properties of An Extracellular Protease of Bacillus Megaterium DSM 319 As Depilating Aid of HidesDocumento6 pagineProperties of An Extracellular Protease of Bacillus Megaterium DSM 319 As Depilating Aid of HidesSarah Fitriani MuzwarNessuna valutazione finora
- IB BIOLOGY SL TOPIC 3 Nucleic Acids & Proteins and Chemical Elements & WaterDocumento13 pagineIB BIOLOGY SL TOPIC 3 Nucleic Acids & Proteins and Chemical Elements & WaterweeNessuna valutazione finora
- KW 15 AbstractsDocumento1.129 pagineKW 15 AbstractsShloime-Batsheva Dalezman100% (1)
- Nonmicrosomal EnzymesDocumento66 pagineNonmicrosomal EnzymesSunil100% (1)
- CI in ConcreteDocumento37 pagineCI in ConcreteMikeNessuna valutazione finora
- Enzyme InhibitionDocumento13 pagineEnzyme InhibitionMheira Villahermosa100% (1)
- Inhibitor Effects of Sodium Benzoate On Corrosion Resistance ofDocumento13 pagineInhibitor Effects of Sodium Benzoate On Corrosion Resistance ofRafi AwanNessuna valutazione finora
- 5 6086852463917269055 PDFDocumento294 pagine5 6086852463917269055 PDFNaveenkumar Neelam100% (1)
- Journal - Dry Fractionation For Sustainable Production of Functional Legumes Protein ConcentrateDocumento9 pagineJournal - Dry Fractionation For Sustainable Production of Functional Legumes Protein ConcentrateFerdian Iwank IriyantoNessuna valutazione finora
- Glycosidase MechanismsDocumento8 pagineGlycosidase MechanismsyNessuna valutazione finora
- SPE 87441 Development of An Enzyme Activated, Low Temperature, Scale Inhibitor Precipitation Squeeze SystemDocumento8 pagineSPE 87441 Development of An Enzyme Activated, Low Temperature, Scale Inhibitor Precipitation Squeeze SystemmsmsoftNessuna valutazione finora
- 44 Enzyme InhibitionDocumento13 pagine44 Enzyme InhibitionMafe HernandezNessuna valutazione finora
- Pengantar Teknologi Desain Obat: H. Muhammad Nur Abdillah, M. Si., AptDocumento89 paginePengantar Teknologi Desain Obat: H. Muhammad Nur Abdillah, M. Si., AptDipperNessuna valutazione finora