Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- HistamineDocumento2 pagineHistamineJulia IshakNessuna valutazione finora
- Venum OrgDocumento3 pagineVenum OrgJulia IshakNessuna valutazione finora
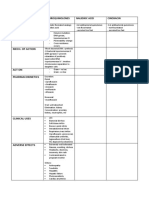
- Aminoglycosides LadscapeDocumento2 pagineAminoglycosides LadscapeJulia IshakNessuna valutazione finora
- Antifolate DrugsDocumento2 pagineAntifolate DrugsJulia IshakNessuna valutazione finora
- Dna Gyrase InhibitorDocumento2 pagineDna Gyrase InhibitorJulia IshakNessuna valutazione finora
- ArthropodsDocumento2 pagineArthropodsJulia IshakNessuna valutazione finora
- AminoglycosidesDocumento2 pagineAminoglycosidesJulia IshakNessuna valutazione finora
- MB Gp2 PassDocumento1 paginaMB Gp2 PassJulia IshakNessuna valutazione finora
- Except in Viruses - May Be RNADocumento6 pagineExcept in Viruses - May Be RNAJulia IshakNessuna valutazione finora
- MB Rickettsiaceae PassDocumento2 pagineMB Rickettsiaceae PassJulia IshakNessuna valutazione finora
- MB GP 4 B& C PassDocumento3 pagineMB GP 4 B& C PassJulia IshakNessuna valutazione finora
- MB Spirochaete PassDocumento2 pagineMB Spirochaete PassJulia IshakNessuna valutazione finora
- Aureus C. Diphteriae (Man) : Classification Based On HaemolysisDocumento4 pagineAureus C. Diphteriae (Man) : Classification Based On HaemolysisJulia IshakNessuna valutazione finora
- ClostridiumDocumento1 paginaClostridiumJulia IshakNessuna valutazione finora
- MB Yeasts PassDocumento1 paginaMB Yeasts PassJulia IshakNessuna valutazione finora
- Bacterial MorphologyDocumento2 pagineBacterial MorphologyJulia IshakNessuna valutazione finora
- Subcutaneous MycosesDocumento1 paginaSubcutaneous MycosesJulia IshakNessuna valutazione finora
- Bacterial Virulence FactorsDocumento2 pagineBacterial Virulence FactorsJulia IshakNessuna valutazione finora
- Normal Body FloraDocumento1 paginaNormal Body FloraJulia IshakNessuna valutazione finora
- Intromycology& DermatophytesDocumento3 pagineIntromycology& DermatophytesJulia IshakNessuna valutazione finora
- Jirovecii: Kingdom: Phylum: Class: Order: Family: Genus: Species: PDocumento4 pagineJirovecii: Kingdom: Phylum: Class: Order: Family: Genus: Species: PJulia IshakNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Classification of Psychiatric DisordersDocumento64 pagineClassification of Psychiatric Disordersdrkadiyala2100% (1)
- Vestibular SchwannomaDocumento12 pagineVestibular SchwannomaEustakia Rini Kartika DewiNessuna valutazione finora
- 2020 11 07 XII Economics 1Documento17 pagine2020 11 07 XII Economics 1Sjft6hd FfNessuna valutazione finora
- Lecture 5 - Facial Pain and TMJ DiseaseDocumento6 pagineLecture 5 - Facial Pain and TMJ DiseaseJeff ChadwickNessuna valutazione finora
- Examinatin in Intensive CareDocumento731 pagineExaminatin in Intensive Careyankee1111100% (1)
- Cultivo Harknessia de EucaliptoDocumento18 pagineCultivo Harknessia de EucaliptoRosales Rosales JesúsNessuna valutazione finora
- Treatment of Sacroiliac Joint DysfunctionDocumento46 pagineTreatment of Sacroiliac Joint DysfunctionMichel Bakker100% (5)
- How The Brain Experiences ArchitectureDocumento16 pagineHow The Brain Experiences ArchitectureAbdu Thora100% (1)
- Jpog August 2013 IdDocumento51 pagineJpog August 2013 IdHasyim PurwadiNessuna valutazione finora
- Phlegmon: by - Dharmendra Singh Group No. - 317Documento15 paginePhlegmon: by - Dharmendra Singh Group No. - 317Mouna Jomaa DhifaouiNessuna valutazione finora
- Alkaloids - Biosynthesis Biological Roles and HealthDocumento285 pagineAlkaloids - Biosynthesis Biological Roles and HealthPrakash PatelNessuna valutazione finora
- Galvano-Spa-Bath and HealthDocumento2 pagineGalvano-Spa-Bath and HealthDeu na telha com Janaína BensdorpNessuna valutazione finora
- Other Products of ChesaDocumento4 pagineOther Products of ChesamikeeNessuna valutazione finora
- Cell DivisionDocumento28 pagineCell DivisionPalagiri MadhuNessuna valutazione finora
- SCHOOL NAME: - Proposed Date and Venue Materials Needed Budget Source Persons/ Offices Involved Expected OutcomesDocumento4 pagineSCHOOL NAME: - Proposed Date and Venue Materials Needed Budget Source Persons/ Offices Involved Expected OutcomesJOLLYBEL GAJWAYENNessuna valutazione finora
- Stroke:: What Should Nurses Need To Know About Stroke?Documento68 pagineStroke:: What Should Nurses Need To Know About Stroke?Suci Aning TNessuna valutazione finora
- Research Presentation Script I. Background of The Study & Introduction of Research TitleDocumento3 pagineResearch Presentation Script I. Background of The Study & Introduction of Research TitleSophia Adel RodriguezNessuna valutazione finora
- SaveBooklet BookletDocumento120 pagineSaveBooklet BookletRoscelie KhoNessuna valutazione finora
- National Medical National Medical Interns' Survey Interns' SurveyDocumento20 pagineNational Medical National Medical Interns' Survey Interns' SurveyKaren Jodes CapananNessuna valutazione finora
- Chapter 1 - A Context For CalculusDocumento7 pagineChapter 1 - A Context For Calculus0169514311Nessuna valutazione finora
- Atlas de AcupunturaDocumento258 pagineAtlas de AcupunturaPatricia Barrera100% (2)
- 2020 Article 773Documento10 pagine2020 Article 773bagas umam alwiNessuna valutazione finora
- Literature Review On Vegetable OilDocumento8 pagineLiterature Review On Vegetable Oilbteubwbnd100% (1)
- Trauma ToraksDocumento30 pagineTrauma ToraksMichael KwanNessuna valutazione finora
- 24.18.00 - Chikungunya2 DR RAGADocumento48 pagine24.18.00 - Chikungunya2 DR RAGAjcvh24Nessuna valutazione finora
- TRS601 Vocabulary ListDocumento5 pagineTRS601 Vocabulary ListNgo Van Hung (K17 HCM)Nessuna valutazione finora
- 3b Oral Exam Practice - Mock Exam THREE - ANSWER Guide PDFDocumento7 pagine3b Oral Exam Practice - Mock Exam THREE - ANSWER Guide PDFJyothsna SridharNessuna valutazione finora
- Giles B1Documento37 pagineGiles B1imgayNessuna valutazione finora
- Fix Daftar PustakaDocumento6 pagineFix Daftar Pustakaeka saptaning windu fitriNessuna valutazione finora
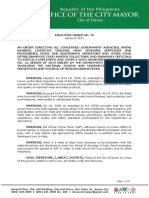
- EO 70 S. 2021 - Movement of Pigs and Pork Products ASF-DSDocumento8 pagineEO 70 S. 2021 - Movement of Pigs and Pork Products ASF-DSJamela SerutNessuna valutazione finora