Potrebbero piacerti anche
- Knowing God: Prayer and Fasting 2013Documento40 pagineKnowing God: Prayer and Fasting 2013ccforgph100% (4)
- RITE Practice QuestionsDocumento28 pagineRITE Practice QuestionsDesiree Mejica100% (2)
- Herbal Abortifacient Drugs A ReviewDocumento6 pagineHerbal Abortifacient Drugs A Reviewyogesh ushirNessuna valutazione finora
- My Study Plan Guide For AmcDocumento7 pagineMy Study Plan Guide For Amc0d&H 8Nessuna valutazione finora
- Pcap Case StudyDocumento7 paginePcap Case StudyArlly Faena AbadNessuna valutazione finora
- M2 Forces and MomentsDocumento46 pagineM2 Forces and MomentsErle100% (1)
- Pediatric Pneumonia Case StudyDocumento44 paginePediatric Pneumonia Case StudyPreiane PayladoNessuna valutazione finora
- Pcap CDocumento32 paginePcap CCess DunwanNessuna valutazione finora
- Introduction To The of The Human Person: PhilosophyDocumento29 pagineIntroduction To The of The Human Person: PhilosophyMarco100% (9)
- J.D.salinger-De Veghe in Lanul de SecaraDocumento14 pagineJ.D.salinger-De Veghe in Lanul de SecaraAnna Lintu Diaconu33% (3)
- PCAP CDocumento42 paginePCAP CJenny YenNessuna valutazione finora
- Architecture of France (Art Ebook)Documento368 pagineArchitecture of France (Art Ebook)elyscribd100% (3)
- University of Northern Philipiens: Republic of The Philippines Tamag, Vigan City 2700, Ilocos SurDocumento25 pagineUniversity of Northern Philipiens: Republic of The Philippines Tamag, Vigan City 2700, Ilocos SurRence Bernard Arde TicaNessuna valutazione finora
- Pedia+smiley Block7Documento7 paginePedia+smiley Block7tej0331Nessuna valutazione finora
- 041+ +1197+ +Peter+Prayogo+Hsieh+ +galleyDocumento4 pagine041+ +1197+ +Peter+Prayogo+Hsieh+ +galleyNaufal JihadNessuna valutazione finora
- Case Study Neonatal SepsisDocumento22 pagineCase Study Neonatal Sepsisaishah shamsudinNessuna valutazione finora
- MCQ FMS 3 (2016) With Answers-1Documento17 pagineMCQ FMS 3 (2016) With Answers-1stella pangestikaNessuna valutazione finora
- General Data: ST ND RDDocumento5 pagineGeneral Data: ST ND RDJill Eizavel BertisNessuna valutazione finora
- Casia Acute RF Sec To PneumoDocumento105 pagineCasia Acute RF Sec To PneumoMarie Ashley CasiaNessuna valutazione finora
- PTB WARD Case Study (CJC-CHS) 2023Documento62 paginePTB WARD Case Study (CJC-CHS) 2023Nil GyiNessuna valutazione finora
- Neonates Hospitalized With Community-Acquired Sars-Cov-2 in A Colorado Neonatal Intensive Care UnitDocumento5 pagineNeonates Hospitalized With Community-Acquired Sars-Cov-2 in A Colorado Neonatal Intensive Care UnitRosario DonosoNessuna valutazione finora
- 13 Areas of AssessmentDocumento3 pagine13 Areas of AssessmentErleNessuna valutazione finora
- Ca Copd (Emphysema)Documento42 pagineCa Copd (Emphysema)Charisse CaydanNessuna valutazione finora
- MIS-C Case Report in 16-Year-Old MaleDocumento19 pagineMIS-C Case Report in 16-Year-Old MaleKamila ArifaNessuna valutazione finora
- Typhoid FeverDocumento38 pagineTyphoid FeverRonelenePurisimaNessuna valutazione finora
- Acute Pancreatitis in Children and Multisystemic Inflammatory Syndrome Post Covid Infection 19Documento6 pagineAcute Pancreatitis in Children and Multisystemic Inflammatory Syndrome Post Covid Infection 19IJAR JOURNALNessuna valutazione finora
- G 3 NCM 122 Lab BSN 4 2 FinalDocumento67 pagineG 3 NCM 122 Lab BSN 4 2 FinalPam RomeroNessuna valutazione finora
- L.case CP1Documento17 pagineL.case CP1aishah shamsudinNessuna valutazione finora
- Journal Reading AnakDocumento19 pagineJournal Reading AnakPutra Priambodo WibowoNessuna valutazione finora
- Catamnesis of Children Covid-19Documento4 pagineCatamnesis of Children Covid-19Central Asian StudiesNessuna valutazione finora
- Clinical Abstract TEMPLATEDocumento3 pagineClinical Abstract TEMPLATEDiannesa April GolosindaNessuna valutazione finora
- CellulitisDocumento121 pagineCellulitisAYTONA, JAMAICA F.Nessuna valutazione finora
- Case ReportDocumento4 pagineCase ReportRegita LatuihamalloNessuna valutazione finora
- Fmab 025Documento9 pagineFmab 025gabopeluditoNessuna valutazione finora
- Caso Clinico NejDocumento9 pagineCaso Clinico NejSilvina MartinezNessuna valutazione finora
- Lesiones Orales Covid19Documento7 pagineLesiones Orales Covid19Diana PerezNessuna valutazione finora
- JCIMCR v3 1706Documento2 pagineJCIMCR v3 1706Mohan ChikkalaNessuna valutazione finora
- 13 Areas of AssessmentDocumento4 pagine13 Areas of AssessmentKryzza LeizellNessuna valutazione finora
- CR Mbak YuliDocumento10 pagineCR Mbak YuliNovel WidyaNessuna valutazione finora
- CR4 - Dea BKDocumento45 pagineCR4 - Dea BKThadea Odilia TandiNessuna valutazione finora
- Pediatric Round PneumoniaDocumento4 paginePediatric Round PneumoniaSalwa Zahra TsamaraNessuna valutazione finora
- BRONCHOPNEUMONIADocumento73 pagineBRONCHOPNEUMONIALizel Roales UrayaniNessuna valutazione finora
- CASE STUDY PSH Hehe 1Documento32 pagineCASE STUDY PSH Hehe 1Mary hope DomalaonNessuna valutazione finora
- First Case of Hemorrhagic Stroke from GBS MeningitisDocumento2 pagineFirst Case of Hemorrhagic Stroke from GBS MeningitisHelen EngelinaNessuna valutazione finora
- B. PathophysiologyDocumento41 pagineB. PathophysiologySergi Lee OrateNessuna valutazione finora
- MainDocumento16 pagineMainOdette SantillánNessuna valutazione finora
- Miliary Tuberculosis With Severe Pneumonia Without Abnormal Chest Sounds in A Covid 19 PandemicDocumento4 pagineMiliary Tuberculosis With Severe Pneumonia Without Abnormal Chest Sounds in A Covid 19 PandemicMelly SyafridaNessuna valutazione finora
- Group 1 Case PresentationDocumento10 pagineGroup 1 Case PresentationAlyssa MasangcayNessuna valutazione finora
- Atypical Hemolytic Uremic Syndrome in A Post-COVID-19 Child: Its Differential Diagnosis With COVID-19, Multisystemic Inflammatory Syndrome and OutcomeDocumento8 pagineAtypical Hemolytic Uremic Syndrome in A Post-COVID-19 Child: Its Differential Diagnosis With COVID-19, Multisystemic Inflammatory Syndrome and OutcomeSandra77777777Nessuna valutazione finora
- Group 38 CaseDocumento73 pagineGroup 38 CaseMarjune DimayugaNessuna valutazione finora
- Paper 1Documento6 paginePaper 1ivan.montenegroNessuna valutazione finora
- PDF TJP 2175Documento5 paginePDF TJP 2175husna fitriaNessuna valutazione finora
- 2 Agn To Be PrintedDocumento115 pagine2 Agn To Be Printedherrabiel solisNessuna valutazione finora
- Articulo 1Documento3 pagineArticulo 1BrendaElielParedesRodriguezNessuna valutazione finora
- Feverinthepediatricpatient: Robyn Wing,, Maya R. Dor,, Patricia A. McquilkinDocumento24 pagineFeverinthepediatricpatient: Robyn Wing,, Maya R. Dor,, Patricia A. McquilkinAzkiaNessuna valutazione finora
- Artikel 1 Inggris Covid-19Documento5 pagineArtikel 1 Inggris Covid-19Fera NurjanahNessuna valutazione finora
- Pcap FinalDocumento51 paginePcap FinalThomas joshua QuiñonesNessuna valutazione finora
- Case Study on 34yo Female with InfluenzaDocumento4 pagineCase Study on 34yo Female with InfluenzaMarjorie EragNessuna valutazione finora
- PEDIA CASE 3 FinalDocumento9 paginePEDIA CASE 3 FinalXandra BnnNessuna valutazione finora
- SARS-CoV-2 Polymorphisms and MIS in ChildrenDocumento7 pagineSARS-CoV-2 Polymorphisms and MIS in ChildrenFeliciaNessuna valutazione finora
- First Aid CaseDocumento9 pagineFirst Aid Caseyunus alfiansahNessuna valutazione finora
- Hematuria As An Early Sign of Multisystem Inflammatory Syndrome in Children: A Case Report of A Boy With Multiple Comorbidities and Review of LiteratureDocumento9 pagineHematuria As An Early Sign of Multisystem Inflammatory Syndrome in Children: A Case Report of A Boy With Multiple Comorbidities and Review of LiteratureDaniel TurudicNessuna valutazione finora
- Case Study_san LazaroDocumento28 pagineCase Study_san LazaroItsMe AJNessuna valutazione finora
- Early hydroxychloroquine and azithromycin therapy for COVID-19Documento8 pagineEarly hydroxychloroquine and azithromycin therapy for COVID-19Tasya OktavianiNessuna valutazione finora
- Neonatal GAS Meningitis Case Report and Literature ReviewDocumento6 pagineNeonatal GAS Meningitis Case Report and Literature ReviewJessyMomoNessuna valutazione finora
- MIDAS Information Technology Co., LTDDocumento2 pagineMIDAS Information Technology Co., LTDErleNessuna valutazione finora
- Midas Gen: 1. Design InformationDocumento1 paginaMidas Gen: 1. Design InformationNyx Phoebe WPNessuna valutazione finora
- MIDAS Information Technology Co., LTDDocumento2 pagineMIDAS Information Technology Co., LTDErleNessuna valutazione finora
- Midas Gen: 1. Design InformationDocumento1 paginaMidas Gen: 1. Design InformationNyx Phoebe WPNessuna valutazione finora
- Midas Gen: 1. Design InformationDocumento1 paginaMidas Gen: 1. Design InformationNyx Phoebe WPNessuna valutazione finora
- Managing Generalized Anxiety Disorder: CBT Intervention for Worrying MotherDocumento20 pagineManaging Generalized Anxiety Disorder: CBT Intervention for Worrying MotherErleNessuna valutazione finora
- Ar 2181 Toa Group 2 FinalDocumento31 pagineAr 2181 Toa Group 2 FinalErleNessuna valutazione finora
- MIDAS Information Technology Co., LTDDocumento6 pagineMIDAS Information Technology Co., LTDErleNessuna valutazione finora
- Reviewer For First Periodical - ABM G12Documento4 pagineReviewer For First Periodical - ABM G12ErleNessuna valutazione finora
- M1 Introduction To StaticsDocumento29 pagineM1 Introduction To StaticsErleNessuna valutazione finora
- When The Word Tax Is MentionedDocumento1 paginaWhen The Word Tax Is MentionedErleNessuna valutazione finora
- Section 1-0 History PDFDocumento202 pagineSection 1-0 History PDF16gamiNessuna valutazione finora
- Section 1-0 History PDFDocumento202 pagineSection 1-0 History PDF16gamiNessuna valutazione finora
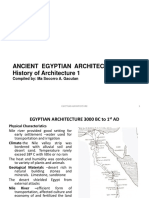
- Ancient Egyptian Architecture History of Architecture 1: Compiled By: Ma Socorro A. GacutanDocumento39 pagineAncient Egyptian Architecture History of Architecture 1: Compiled By: Ma Socorro A. GacutanDenzel NgNessuna valutazione finora
- Sample ResumeDocumento3 pagineSample ResumeMaribelNessuna valutazione finora
- Architectural Lettering StyleDocumento3 pagineArchitectural Lettering StyleAnnhe BucalNessuna valutazione finora
- Architecture Portfolio - by SlidesgoDocumento84 pagineArchitecture Portfolio - by Slidesgobibe retro sablonNessuna valutazione finora
- Villa SavoyeDocumento2 pagineVilla SavoyeErleNessuna valutazione finora
- Year Carson BibliaDocumento2 pagineYear Carson BibliaRamon M. SosaNessuna valutazione finora
- Licensed To Plumb: Audio AlternativeDocumento2 pagineLicensed To Plumb: Audio AlternativeErleNessuna valutazione finora
- VILLA SAVOYE - Architecture of France by David A. HanserDocumento7 pagineVILLA SAVOYE - Architecture of France by David A. HanserErleNessuna valutazione finora
- What Is Brno? FunctionalismDocumento50 pagineWhat Is Brno? FunctionalismErleNessuna valutazione finora
- The Study of The Influence of FunctionalDocumento10 pagineThe Study of The Influence of FunctionalErleNessuna valutazione finora
- Notes TemplateDocumento1 paginaNotes TemplateErleNessuna valutazione finora
- Module 1: Introduction To Fashion DesignDocumento1 paginaModule 1: Introduction To Fashion DesignErleNessuna valutazione finora
- Architecture Portfolio - by SlidesgoDocumento84 pagineArchitecture Portfolio - by Slidesgobibe retro sablonNessuna valutazione finora
- Sheet 01Documento1 paginaSheet 01Rajeshwari YeoleNessuna valutazione finora
- Step by Step To The Perfect PedicureDocumento6 pagineStep by Step To The Perfect PedicurepinkyNessuna valutazione finora
- LESSON 2 - TRANSMUTATION - Louise Peralta - 11 - FairnessDocumento2 pagineLESSON 2 - TRANSMUTATION - Louise Peralta - 11 - FairnessLouise Joseph PeraltaNessuna valutazione finora
- Solution Manual For Safety Health and Environmental Concepts For The Process Industry 2nd EditionDocumento8 pagineSolution Manual For Safety Health and Environmental Concepts For The Process Industry 2nd EditionRobert Hornback100% (34)
- Buttermilk and Ghee ResidueDocumento15 pagineButtermilk and Ghee ResidueRonak RawatNessuna valutazione finora
- Pidato Bahasa InggrisDocumento4 paginePidato Bahasa InggrisAriya Manikmaya100% (1)
- WILLIEEMS TIBLANI - NURS10 Student Copy Module 15 Part1Documento32 pagineWILLIEEMS TIBLANI - NURS10 Student Copy Module 15 Part1Toyour EternityNessuna valutazione finora
- F6003 5W40 Synthetic Oil Technical Data SheetDocumento1 paginaF6003 5W40 Synthetic Oil Technical Data SheetValeriy ValkovetsNessuna valutazione finora
- Dasar Genetik GandumDocumento282 pagineDasar Genetik GandumAlekkyNessuna valutazione finora
- Sohail KhanDocumento3 pagineSohail KhanRashid Muhammad SarwarNessuna valutazione finora
- AP000100 EngDocumento9 pagineAP000100 EngLucas WrightNessuna valutazione finora
- Biochips Combine A Triad of Micro-Electro-Mechanical, Biochemical, and Photonic TechnologiesDocumento5 pagineBiochips Combine A Triad of Micro-Electro-Mechanical, Biochemical, and Photonic TechnologiesDinesh KumarNessuna valutazione finora
- GarrettDocumento2 pagineGarrettAndrey MarviantoNessuna valutazione finora
- Face SerumDocumento10 pagineFace SerumLiliana CojocaruNessuna valutazione finora
- The Baking and Frozen Dough MarketDocumento4 pagineThe Baking and Frozen Dough MarketMilling and Grain magazineNessuna valutazione finora
- Liu030 Nepal Bans Solo Mountain ClimbersDocumento2 pagineLiu030 Nepal Bans Solo Mountain Climberssanti.miranda.parrillaNessuna valutazione finora
- Guillermo Waco v. People Homicide RulingDocumento1 paginaGuillermo Waco v. People Homicide RulingCandelaria QuezonNessuna valutazione finora
- Form-Ii (See Regulation 4) Postal Bill of Export - II (To Be Submitted in Duplicate)Documento1 paginaForm-Ii (See Regulation 4) Postal Bill of Export - II (To Be Submitted in Duplicate)mrthilagamNessuna valutazione finora
- Deped Memo No. 165, S 2010: WastedDocumento6 pagineDeped Memo No. 165, S 2010: WastedJayne InoferioNessuna valutazione finora
- Waste Management: Spoilage of LandscapeDocumento7 pagineWaste Management: Spoilage of Landscapeshauryasahu2004Nessuna valutazione finora
- Análisis de Estabilidad de TaludesDocumento4 pagineAnálisis de Estabilidad de TaludesJosue Acosta EspinozaNessuna valutazione finora
- R02.4 Standard III (A) - AnswersDocumento11 pagineR02.4 Standard III (A) - AnswersShashwat DesaiNessuna valutazione finora
- The Evolution of FungiDocumento15 pagineThe Evolution of Fungi2010eon2010Nessuna valutazione finora
- (L-2) - Cell - Mar 03, 2020Documento52 pagine(L-2) - Cell - Mar 03, 2020puneetlokwani04Nessuna valutazione finora
- Series NRX With PXR - Type NF Low Voltage Power (Air) Circuit Breaker Instruction ManualDocumento70 pagineSeries NRX With PXR - Type NF Low Voltage Power (Air) Circuit Breaker Instruction ManualHamilton GutierrezNessuna valutazione finora
- The Design of The 2016-17 Young Lives School Survey in EthiopiaDocumento10 pagineThe Design of The 2016-17 Young Lives School Survey in EthiopiaFuadNessuna valutazione finora
- Definitions of Abnormality by Dr. Kanwal QadeerDocumento7 pagineDefinitions of Abnormality by Dr. Kanwal QadeerHaya EishaNessuna valutazione finora