Potrebbero piacerti anche
- Brain ImagesDocumento24 pagineBrain Imagesmemoumou27Nessuna valutazione finora
- Complete Blood Count Pt. 1 (Module-Based)Documento5 pagineComplete Blood Count Pt. 1 (Module-Based)Iya BangalanNessuna valutazione finora
- RBC WBC Nebuer ChambarDocumento58 pagineRBC WBC Nebuer ChambarABHINABA GUPTANessuna valutazione finora
- A. Lag PhaseDocumento16 pagineA. Lag PhaseMarry Grace CiaNessuna valutazione finora
- The Complete Guide To Vascular Ultrasound PDFDocumento146 pagineThe Complete Guide To Vascular Ultrasound PDFAnna Sofía ParedesNessuna valutazione finora
- Dr. Agtuca - PBS, Differential Count, and Reticulocyte CountDocumento58 pagineDr. Agtuca - PBS, Differential Count, and Reticulocyte Countمصطفي خندقاويNessuna valutazione finora
- Blood InvestigationDocumento70 pagineBlood InvestigationRohit RaiNessuna valutazione finora
- MCQs For Essentials of Oral Histology and Embryology (2015) PDFDocumento199 pagineMCQs For Essentials of Oral Histology and Embryology (2015) PDFLokesh Bakshi100% (1)
- Metodo, Entrenamiento y Principios Del ADVIA 120Documento64 pagineMetodo, Entrenamiento y Principios Del ADVIA 120Jaime Elias100% (3)
- Lecture2 GranulopoiesisDocumento9 pagineLecture2 GranulopoiesisAfifa Prima GittaNessuna valutazione finora
- Urinary System PDFDocumento27 pagineUrinary System PDFfiona100% (3)
- Nca HematologyDocumento23 pagineNca HematologyMariel CalimlimNessuna valutazione finora
- Manual CBC 1 3: - Wbcs - Platelets Count - PCV or HCT - Retics Count - HB Estimation 3 3 4 5 6Documento25 pagineManual CBC 1 3: - Wbcs - Platelets Count - PCV or HCT - Retics Count - HB Estimation 3 3 4 5 6Aqila MumtazNessuna valutazione finora
- Test No.: 012 008 B2 StencilDocumento2 pagineTest No.: 012 008 B2 StencilCalvawell Muzvondiwa100% (7)
- Blood & Blood ProductsDocumento126 pagineBlood & Blood ProductsdrprasadingleyNessuna valutazione finora
- Chapter 2.0 Cell Signalling and Endocrine RegulationDocumento93 pagineChapter 2.0 Cell Signalling and Endocrine RegulationNurarief AffendyNessuna valutazione finora
- 150 Question Labce Quez. 1 PDFDocumento87 pagine150 Question Labce Quez. 1 PDFadvance ascpNessuna valutazione finora
- Dictyosome: Modifying, and Packaging Proteins and Lipids Into Vesicles ForDocumento11 pagineDictyosome: Modifying, and Packaging Proteins and Lipids Into Vesicles ForASHFAQ AHMAD100% (1)
- Basic Hematologic TestsDocumento9 pagineBasic Hematologic TestsdtimtimanNessuna valutazione finora
- HematologyDocumento158 pagineHematologyKrisyah Niqoule Valdez67% (3)
- Platelet Count NotesDocumento6 paginePlatelet Count Notesangelina buenaNessuna valutazione finora
- Hematology: Presented by Alyazeed Hussein, BSCDocumento96 pagineHematology: Presented by Alyazeed Hussein, BSCMONFOLANessuna valutazione finora
- Transfusion Medicine and Hemostasis: Clinical and Laboratory AspectsDa EverandTransfusion Medicine and Hemostasis: Clinical and Laboratory AspectsValutazione: 4 su 5 stelle4/5 (9)
- RBC CountsDocumento16 pagineRBC Countsalmastar officeNessuna valutazione finora
- Hematological: TestsDocumento40 pagineHematological: Testspupun8965Nessuna valutazione finora
- Clinical Haematology Lab. 1: Practical PhysiologyDocumento31 pagineClinical Haematology Lab. 1: Practical PhysiologyHameed SabahNessuna valutazione finora
- Plasma Hemoglobin and Urine Hemoglobin EstimationDocumento12 paginePlasma Hemoglobin and Urine Hemoglobin EstimationAvi VermaNessuna valutazione finora
- Clinical For PracticalDocumento72 pagineClinical For PracticalYogendra SinghNessuna valutazione finora
- Basic Examinations of The Blood: 0.5G SHB/DL of Blood O Hemoglobin Concentration DeterminationDocumento14 pagineBasic Examinations of The Blood: 0.5G SHB/DL of Blood O Hemoglobin Concentration DeterminationZllison Mae Teodoro MangabatNessuna valutazione finora
- Routine Hematological InvestigationsDocumento62 pagineRoutine Hematological InvestigationsDarshan GohilNessuna valutazione finora
- Harr ReviewerDocumento5 pagineHarr ReviewerBernard Garcia OledanNessuna valutazione finora
- Hemoglobin Determination: Cyanmethemoglobin MethodDocumento32 pagineHemoglobin Determination: Cyanmethemoglobin MethodNasser DabiNessuna valutazione finora
- Introduction of Natural ImmunityDocumento4 pagineIntroduction of Natural ImmunitySamanthaNessuna valutazione finora
- Anemia, Tic, DLC MbbsDocumento50 pagineAnemia, Tic, DLC Mbbssharads221004Nessuna valutazione finora
- HematocritDocumento3 pagineHematocritMaybelle Acap PatnubayNessuna valutazione finora
- Hematolgy ReviewDocumento4 pagineHematolgy Reviewweiwei WangNessuna valutazione finora
- Hematology 1 (Laboratory) - Week 10-11 ModuleDocumento8 pagineHematology 1 (Laboratory) - Week 10-11 ModuleJam RamosNessuna valutazione finora
- 4 Blood ProductsDocumento11 pagine4 Blood ProductsGampa VijaykumarNessuna valutazione finora
- 2814 1Documento73 pagine2814 1Trangia, SharmaineNessuna valutazione finora
- Hemolytic Anemia - Part 1 PDFDocumento11 pagineHemolytic Anemia - Part 1 PDFادم PrabowoNessuna valutazione finora
- Practical HB HV (Physiology)Documento29 paginePractical HB HV (Physiology)Madonna Hany naeemNessuna valutazione finora
- HEMA LAB Reticulocyte Study ESR OFT RBC CountDocumento17 pagineHEMA LAB Reticulocyte Study ESR OFT RBC CountJam RamosNessuna valutazione finora
- 2023.LabDx - Trans01.basic Examination of BloodDocumento4 pagine2023.LabDx - Trans01.basic Examination of BloodstellaNessuna valutazione finora
- Manual Hematological Procedures Frequently Forgotten Concepts and MethodologiesDocumento8 pagineManual Hematological Procedures Frequently Forgotten Concepts and MethodologiesWynlor AbarcaNessuna valutazione finora
- Blood & Blood Products OnlyDocumento54 pagineBlood & Blood Products OnlydrprasadingleyNessuna valutazione finora
- Hema FIN NotesDocumento8 pagineHema FIN NotessansastarkNessuna valutazione finora
- Hema Lab MidtermDocumento130 pagineHema Lab MidtermTrangia, SharmaineNessuna valutazione finora
- Section 13 - Hematology (Updated)Documento34 pagineSection 13 - Hematology (Updated)Lorelie CarlosNessuna valutazione finora
- OriginalhematologyDocumento56 pagineOriginalhematologyShahid HussainNessuna valutazione finora
- Blood Products. Preparation of Blood ComponentsDocumento32 pagineBlood Products. Preparation of Blood ComponentsSanthiya MadhavanNessuna valutazione finora
- HemoglobindeterminationDocumento24 pagineHemoglobindeterminationLiazq0% (2)
- Esr 2023Documento9 pagineEsr 2023Ahmed momtazZzNessuna valutazione finora
- Haematology 2 ManualDocumento26 pagineHaematology 2 Manualhayamitib11Nessuna valutazione finora
- Dav N Haematology LNDocumento10 pagineDav N Haematology LNchittsat3961Nessuna valutazione finora
- HAEMATOLOGYDocumento21 pagineHAEMATOLOGYNéronNessuna valutazione finora
- Perioperative Fluid Therapy: Department of Anesthesiology &ICU KKUH. King Saud UniversityDocumento47 paginePerioperative Fluid Therapy: Department of Anesthesiology &ICU KKUH. King Saud Universityarifjo7999Nessuna valutazione finora
- WBC Count: RBC Count, HB, HCT, Blood Indices WBC Count & PLT CountDocumento36 pagineWBC Count: RBC Count, HB, HCT, Blood Indices WBC Count & PLT CountppcarpediemNessuna valutazione finora
- 1472 - Practical 2 - Total RBC Count by Hemocytometer - Hematology PracticalsDocumento8 pagine1472 - Practical 2 - Total RBC Count by Hemocytometer - Hematology PracticalsnihaNessuna valutazione finora
- 2LAB1Documento29 pagine2LAB1علي صفاء عبد الزهرهNessuna valutazione finora
- Haemocytometry-WPS OfficeDocumento4 pagineHaemocytometry-WPS OfficePrince Raj SinhaNessuna valutazione finora
- Hema Quiz RatioDocumento20 pagineHema Quiz RatioElla OrtegaNessuna valutazione finora
- Special Hematologic ExaminationDocumento5 pagineSpecial Hematologic ExaminationdtimtimanNessuna valutazione finora
- Reviewer Hema LabDocumento12 pagineReviewer Hema LabPatricia Jean RodriguezNessuna valutazione finora
- Hematology Set BDocumento21 pagineHematology Set BJulien Mae GalangNessuna valutazione finora
- Laboratory Approach To AnemiasDocumento23 pagineLaboratory Approach To AnemiasDr. Ashish JawarkarNessuna valutazione finora
- Hematology Lecture Lesson 1&2Documento3 pagineHematology Lecture Lesson 1&2puhtaytoeNessuna valutazione finora
- Test 10 PDFDocumento2 pagineTest 10 PDFLarona SivakoNessuna valutazione finora
- Final Test 4Documento14 pagineFinal Test 4Larona SivakoNessuna valutazione finora
- Final Test 7-ReviewDocumento2 pagineFinal Test 7-ReviewLarona SivakoNessuna valutazione finora
- Test 1 Stencil-1Documento2 pagineTest 1 Stencil-1Larona SivakoNessuna valutazione finora
- Final Test 8Documento2 pagineFinal Test 8Larona SivakoNessuna valutazione finora
- Test 3 StencilDocumento2 pagineTest 3 StencilLarona SivakoNessuna valutazione finora
- SplenectomyDocumento69 pagineSplenectomyAgita GintingNessuna valutazione finora
- Gi PhysiologyDocumento21 pagineGi PhysiologyNoreen Orro BernalNessuna valutazione finora
- Control and CoordinationDocumento15 pagineControl and CoordinationHARSH AKSHIT (B15CS018)Nessuna valutazione finora
- LORESCA - BB Ratio Activity 2Documento14 pagineLORESCA - BB Ratio Activity 2Kaycee Gretz LorescaNessuna valutazione finora
- Group No. Date Performed Name Date Submitted Facilitator ScoreDocumento7 pagineGroup No. Date Performed Name Date Submitted Facilitator ScoreYancy BagsaoNessuna valutazione finora
- HistopathDocumento37 pagineHistopathFait HeeNessuna valutazione finora
- Histology Lecture #2Documento9 pagineHistology Lecture #2رشيد عليانNessuna valutazione finora
- Cells Worksheet 2022Documento2 pagineCells Worksheet 2022Mariah CampbellNessuna valutazione finora
- Aristotle S Anatomical Philosophy of NatureDocumento29 pagineAristotle S Anatomical Philosophy of NatureManuel AvataresNessuna valutazione finora
- Histology of Male Reproductive SystemDocumento56 pagineHistology of Male Reproductive SystemMuhammad Irfan100% (2)
- Case Report: Total Lower Eyelid Reconstruction With A Prefabricated Flap Using Auricular CartilageDocumento7 pagineCase Report: Total Lower Eyelid Reconstruction With A Prefabricated Flap Using Auricular CartilageFaisal HameedNessuna valutazione finora
- How Do Phagocytes Work in The BodyDocumento2 pagineHow Do Phagocytes Work in The Bodykei04086100% (1)
- Renal OsteodistrophyDocumento18 pagineRenal OsteodistrophyFadlan ADima AdriantaNessuna valutazione finora
- Module 2 - AntepartumDocumento3 pagineModule 2 - Antepartumjuancho balandraNessuna valutazione finora
- Cell PartsDocumento2 pagineCell PartsZarahbeth Claire G. ArcederaNessuna valutazione finora
- Jove-84-51214 - Vasectomy, Mouse ModelDocumento8 pagineJove-84-51214 - Vasectomy, Mouse ModelGia KuteliaNessuna valutazione finora
- 9.intracellular Accumulations 1Documento45 pagine9.intracellular Accumulations 1Ramesh KumarNessuna valutazione finora
- Chapter 4Documento21 pagineChapter 4muhammad syamimNessuna valutazione finora
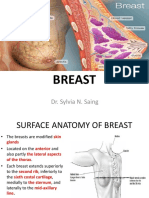
- Breast: Dr. Sylvia N. SaingDocumento26 pagineBreast: Dr. Sylvia N. SaingRichard 151289100% (1)
- Science-F-1-Unit-3 - Cells and Human ReproductionDocumento12 pagineScience-F-1-Unit-3 - Cells and Human ReproductionLong yiu ChanNessuna valutazione finora
- Animal NutritionDocumento16 pagineAnimal NutritionShop AliceNessuna valutazione finora
- Basicinterpretationofcxr 110913060449 Phpapp01Documento84 pagineBasicinterpretationofcxr 110913060449 Phpapp01Alexandra DîrțuNessuna valutazione finora