Potrebbero piacerti anche
- The Ultimate IGCSE Guide To BiologyDocumento53 pagineThe Ultimate IGCSE Guide To BiologyAbdul Raheem100% (1)
- CKD Pocket GuideDocumento2 pagineCKD Pocket GuideLutfi MalefoNessuna valutazione finora
- Anemia ChartDocumento1 paginaAnemia ChartBetsy Brown ByersmithNessuna valutazione finora
- SOAP Note Example 32 Weeks OB CheckDocumento4 pagineSOAP Note Example 32 Weeks OB CheckG. Crusor-PriceNessuna valutazione finora
- Test Bank Lehne S Pharmacotherapeutics For Advanced Practice Nurses and Physician Assistants 2nd EdiDocumento479 pagineTest Bank Lehne S Pharmacotherapeutics For Advanced Practice Nurses and Physician Assistants 2nd EdiBetsy Brown Byersmith89% (133)
- Care PlanDocumento11 pagineCare PlanAlyssa Cardinal100% (1)
- Pulmonary Patho PDFDocumento623 paginePulmonary Patho PDFNabeel Shahzad100% (1)
- Advanced Pharmacology Module 4 DiscussionDocumento3 pagineAdvanced Pharmacology Module 4 Discussionapi-634345342Nessuna valutazione finora
- CardiacDocumento10 pagineCardiacMarcus Reynolds100% (1)
- Anti-Arrhythmic Agents For Pharmacy PDFDocumento41 pagineAnti-Arrhythmic Agents For Pharmacy PDFKelvinTMaikanaNessuna valutazione finora
- Pharmacology ReviewDocumento64 paginePharmacology ReviewRichard BakerNessuna valutazione finora
- Exam 1 Study Guide Summary Advanced Health AssessmentDocumento27 pagineExam 1 Study Guide Summary Advanced Health AssessmentRhoda Mae Cubilla100% (1)
- Clinical Lab Guide: by MedgeeksDocumento17 pagineClinical Lab Guide: by MedgeeksHuy HoangNessuna valutazione finora
- Family Medicine M3 Clerkship Hypertensive Disorders: Joy Shen-Wagner MDDocumento35 pagineFamily Medicine M3 Clerkship Hypertensive Disorders: Joy Shen-Wagner MDJT ThomasNessuna valutazione finora
- Cardiology Teaching PackageDocumento9 pagineCardiology Teaching PackageRicy SaiteNessuna valutazione finora
- Cardiovascular Agents Group 1 Parmacology ReportingDocumento415 pagineCardiovascular Agents Group 1 Parmacology ReportingMajestic RavenNessuna valutazione finora
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNessuna valutazione finora
- Hepatorenal Syndrome: Causes, Tests, and Treatment OptionsDa EverandHepatorenal Syndrome: Causes, Tests, and Treatment OptionsValutazione: 4.5 su 5 stelle4.5/5 (2)
- A. Inflammation and Repair: I. Disease Process (6 Questions)Documento17 pagineA. Inflammation and Repair: I. Disease Process (6 Questions)Anonymous Sw4Pk9fNessuna valutazione finora
- Medical Review of Systems: General, Constitutional Heart and Cardiovascular Hematologic/LymphaticDocumento1 paginaMedical Review of Systems: General, Constitutional Heart and Cardiovascular Hematologic/LymphaticBola S-SNessuna valutazione finora
- Treatment of Resistant and Refractory HypertensionDocumento21 pagineTreatment of Resistant and Refractory HypertensionLuis Rodriguez100% (1)
- Assessment of The Acutely Ill PatientDocumento10 pagineAssessment of The Acutely Ill PatientZacmilo Dela TorreNessuna valutazione finora
- Top-200-Drug ETSYDocumento31 pagineTop-200-Drug ETSYBetsy Brown ByersmithNessuna valutazione finora
- Mksap 19 NeurologyDocumento172 pagineMksap 19 NeurologyNimer Abdelhadi AliNessuna valutazione finora
- Neuro Notes #3Documento11 pagineNeuro Notes #3Monica JubaneNessuna valutazione finora
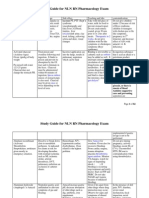
- Advanced Pharmacology Study Guide II PDFDocumento77 pagineAdvanced Pharmacology Study Guide II PDFBetsy Brown Byersmith100% (1)
- Bates Physical Examination RED NOTESDocumento2 pagineBates Physical Examination RED NOTESAmanda Gomez100% (1)
- Assessment of The Chest and LungsDocumento46 pagineAssessment of The Chest and LungsSumathi GopinathNessuna valutazione finora
- Stroke - Final ReportDocumento16 pagineStroke - Final ReportgolokipokNessuna valutazione finora
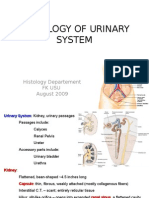
- K2 - Histology of Urinary SystemDocumento46 pagineK2 - Histology of Urinary SystemAnonymous EzxZg4uQ63100% (2)
- All Quiz QuestionsDocumento60 pagineAll Quiz QuestionsMorgan ChristNessuna valutazione finora
- History Taking and Physical Examination of Cardiovascular System-The EssentialsDocumento72 pagineHistory Taking and Physical Examination of Cardiovascular System-The EssentialsReena Joanella TimbreNessuna valutazione finora
- Advanced Pharm From QuizletDocumento62 pagineAdvanced Pharm From QuizletBetsy Brown Byersmith100% (1)
- Mechanical VentilationDocumento43 pagineMechanical VentilationsalemraghuNessuna valutazione finora
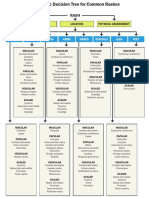
- WK 5 Rash Decision TreeDocumento1 paginaWK 5 Rash Decision TreeBetsy Brown ByersmithNessuna valutazione finora
- Family Medicine 33: 28-Year-Old Female With Dizziness: Learning ObjectivesDocumento6 pagineFamily Medicine 33: 28-Year-Old Female With Dizziness: Learning ObjectivesAndrea Kristin OrigenesNessuna valutazione finora
- Guidelines For Complete SOAP2Documento2 pagineGuidelines For Complete SOAP2Betsy Brown Byersmith100% (1)
- PANCE Prep Pearls Valvular Disease PDFDocumento4 paginePANCE Prep Pearls Valvular Disease PDFkatNessuna valutazione finora
- N5315 Advanced Pathophysiology Syllabus Fall 2014Documento15 pagineN5315 Advanced Pathophysiology Syllabus Fall 2014meeeh100% (1)
- Hepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandHepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- 6521 Advanced Pharmacology Final ExamDocumento19 pagine6521 Advanced Pharmacology Final ExamSandra JeffersonNessuna valutazione finora
- GI PathoDocumento20 pagineGI Pathojutah2013Nessuna valutazione finora
- Anemia HemoliticaDocumento14 pagineAnemia Hemoliticadahiana madrid quinteroNessuna valutazione finora
- Mood Disorders: Advanced Practice Education AssociatesDocumento11 pagineMood Disorders: Advanced Practice Education AssociatesAndrea100% (1)
- AHP - Family Nurse PractitionerDocumento6 pagineAHP - Family Nurse PractitionerMaria Fudji HastutiNessuna valutazione finora
- C 37Documento9 pagineC 37Tammie Gore100% (3)
- Seidels P.E Chapter 5 Test BankDocumento5 pagineSeidels P.E Chapter 5 Test BankAthena Saturday100% (1)
- Hyponatremia, (Low Blood Sodium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandHyponatremia, (Low Blood Sodium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- NURSING Review Session (Nur 220) Part 1Documento8 pagineNURSING Review Session (Nur 220) Part 1Mariel EstoniloNessuna valutazione finora
- Clinical Microscopy Technical ManualDocumento10 pagineClinical Microscopy Technical ManualSharon ChuaNessuna valutazione finora
- Diagnostic Pathology Kidney Diseases 3Rd Edition Full ChapterDocumento41 pagineDiagnostic Pathology Kidney Diseases 3Rd Edition Full Chapterrobert.burge405100% (27)
- Viii. PathophysiologyDocumento2 pagineViii. Pathophysiologymacedon145377Nessuna valutazione finora
- TestBank Norris Porths Essentials Pathophysiology 5e 2019Documento505 pagineTestBank Norris Porths Essentials Pathophysiology 5e 2019Cindy Perez0% (1)
- Nephrology Certification Examination Blueprint - American Board of Internal MedicineDocumento4 pagineNephrology Certification Examination Blueprint - American Board of Internal MedicineabimorgNessuna valutazione finora
- Swollen Kidney, (Hydronephrosis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandSwollen Kidney, (Hydronephrosis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Pathophysiology 2Documento92 paginePathophysiology 2Princess AgarwalNessuna valutazione finora
- Cardiac (Heart) FailureDocumento27 pagineCardiac (Heart) FailureSanthoshi Sadhanaa SankarNessuna valutazione finora
- 351-Discussion Board 2Documento2 pagine351-Discussion Board 2api-546070989Nessuna valutazione finora
- ECG Rhythm Strip Interpretation Lesson 4Documento5 pagineECG Rhythm Strip Interpretation Lesson 4phoebjaetanNessuna valutazione finora
- O Insert Picture Here From Slide: Heart Failure Heart FailureDocumento4 pagineO Insert Picture Here From Slide: Heart Failure Heart FailureAlec Xavier MirandaNessuna valutazione finora
- Patho 3Documento11 paginePatho 3Dranreb Berylle MasangkayNessuna valutazione finora
- Bate's Guide To Physical examination+MCQsDocumento4 pagineBate's Guide To Physical examination+MCQsRaden Adjeng PalupiNessuna valutazione finora
- Edmunds & Mayhew Advanced Pharmacology Chapter 1 Test BankDocumento2 pagineEdmunds & Mayhew Advanced Pharmacology Chapter 1 Test BankHunter HuntingtongNessuna valutazione finora
- Surgery Tips and ResourcesDocumento2 pagineSurgery Tips and ResourcesAbeebs SalahouNessuna valutazione finora
- 2011 Understanding Pharmacology Essentials For Medication SafetyDocumento1 pagina2011 Understanding Pharmacology Essentials For Medication SafetygloriyaNessuna valutazione finora
- Renal Transplant: 1) Steps Involved in Kidney TransplantationDocumento4 pagineRenal Transplant: 1) Steps Involved in Kidney TransplantationNadia SalwaniNessuna valutazione finora
- Medical Surgical QuizDocumento12 pagineMedical Surgical QuizLyka DimayacyacNessuna valutazione finora
- Hypernatremia From HarrisonDocumento3 pagineHypernatremia From HarrisonNobel LaureateNessuna valutazione finora
- This Study Resource Was: G R A D E S L A B - C O MDocumento8 pagineThis Study Resource Was: G R A D E S L A B - C O MHugsNessuna valutazione finora
- 6 Kuliah Liver CirrhosisDocumento55 pagine6 Kuliah Liver CirrhosisAnonymous vUEDx8100% (1)
- C 2Documento12 pagineC 2Tammie Gore100% (4)
- Pathophysiology Exam 4 - ReviewDocumento18 paginePathophysiology Exam 4 - ReviewWaqas GillNessuna valutazione finora
- Critical Care NursingDocumento85 pagineCritical Care NursinganreilegardeNessuna valutazione finora
- AcutePrescribingLimits FINALDocumento1 paginaAcutePrescribingLimits FINALBetsy Brown ByersmithNessuna valutazione finora
- Cardiovascular System SheetDocumento11 pagineCardiovascular System SheetBetsy Brown ByersmithNessuna valutazione finora
- Cardiovascular System SheetDocumento11 pagineCardiovascular System SheetBetsy Brown ByersmithNessuna valutazione finora
- DRUG Card FormDocumento4 pagineDRUG Card FormBetsy Brown ByersmithNessuna valutazione finora
- 2018 Aha/Acc/Aacvpr/Aapa/Abc/Acpm/Ada/Ags/Apha/Aspc/Nla/Pcna Guideline On The Management of Blood Cholesterol: Executive SummaryDocumento77 pagine2018 Aha/Acc/Aacvpr/Aapa/Abc/Acpm/Ada/Ags/Apha/Aspc/Nla/Pcna Guideline On The Management of Blood Cholesterol: Executive SummaryBetsy Brown ByersmithNessuna valutazione finora
- A2-Questions On Analyzing Nutrition ClaimsDocumento3 pagineA2-Questions On Analyzing Nutrition ClaimsBetsy Brown ByersmithNessuna valutazione finora
- Chemistry I The Atomic Bomb Elizabeth Byersmith February 26, 2009 Mercy College Professor KinglseyDocumento3 pagineChemistry I The Atomic Bomb Elizabeth Byersmith February 26, 2009 Mercy College Professor KinglseyBetsy Brown ByersmithNessuna valutazione finora
- What Are Analgesics?Documento10 pagineWhat Are Analgesics?Betsy Brown ByersmithNessuna valutazione finora
- Filtracion GlomerularDocumento18 pagineFiltracion GlomerularNicole Jheny Raraz SosaNessuna valutazione finora
- Urinary System-1Documento48 pagineUrinary System-1Muhammad SajjadNessuna valutazione finora
- Diabetic NephropathyDocumento7 pagineDiabetic NephropathyPlot BUnniesNessuna valutazione finora
- Chronic Kidney DiseaseDocumento39 pagineChronic Kidney DiseaseMohmmadRjab SederNessuna valutazione finora
- Renal FunctionDocumento4 pagineRenal FunctionCoralene Rose SilverioNessuna valutazione finora
- LP AnsDocumento16 pagineLP AnsGayatri MishraNessuna valutazione finora
- Chapter 12 - Urinary SystemDocumento50 pagineChapter 12 - Urinary SystemynaNessuna valutazione finora
- Excellup Class TenDocumento3 pagineExcellup Class TenHemant KumarNessuna valutazione finora
- Pharmacology MCQS1Documento11 paginePharmacology MCQS1Y Sp2Nessuna valutazione finora
- Pa Essentials of Clinical Pathology 2010 PDF UnitedvrgDocumento382 paginePa Essentials of Clinical Pathology 2010 PDF UnitedvrgSafdar Ali67% (3)
- The Urinary System: Essentials of Human Anatomy & PhysiologyDocumento47 pagineThe Urinary System: Essentials of Human Anatomy & Physiologyteu doongieNessuna valutazione finora
- "Nephrotic Syndrome": Case ReportDocumento30 pagine"Nephrotic Syndrome": Case ReportRisa Maulida WidjayaNessuna valutazione finora
- ACOG Practice Bulletin No 202 Gestational.49Documento25 pagineACOG Practice Bulletin No 202 Gestational.49Diana Enco MurillosNessuna valutazione finora
- Urinary System LabDocumento2 pagineUrinary System LabMaria Pearlita TanNessuna valutazione finora
- Krok 1 Medicine: Test Items For Licensing ExaminationDocumento24 pagineKrok 1 Medicine: Test Items For Licensing ExaminationMarinaNessuna valutazione finora
- 6 Krok GitDocumento14 pagine6 Krok GitRodriguez Vivanco Kevin DanielNessuna valutazione finora
- Urinary SystemDocumento5 pagineUrinary SystemDonnabell DayudayNessuna valutazione finora
- Rabia Ali Final - UPDATED VersionDocumento9 pagineRabia Ali Final - UPDATED VersionAamir Bugti50% (2)
- Cambridge International AS & A Level: Biology 9700/42 October/November 2021Documento24 pagineCambridge International AS & A Level: Biology 9700/42 October/November 2021lllllisaNessuna valutazione finora
- Biokimia Urine, Sisa Metabolisme Dan Pembentukan BatuDocumento104 pagineBiokimia Urine, Sisa Metabolisme Dan Pembentukan BatuHenny Taufik GosalNessuna valutazione finora
- Kidney NewDocumento4 pagineKidney NewParth BhayanaNessuna valutazione finora
- BBM - 978 3 319 23458 8/1 PDFDocumento22 pagineBBM - 978 3 319 23458 8/1 PDFmedicalNessuna valutazione finora
- NephritisDocumento16 pagineNephritisyikesNessuna valutazione finora
- 5.01 Urinary System: I. A. B. II. Iii. IV. A. B. C. D. E. V. VI. ViiDocumento10 pagine5.01 Urinary System: I. A. B. II. Iii. IV. A. B. C. D. E. V. VI. ViiKarsten SolasNessuna valutazione finora