Potrebbero piacerti anche
- Jurnal 1Documento11 pagineJurnal 1izal yusufNessuna valutazione finora
- A Medical Director's PerspectiveDocumento4 pagineA Medical Director's Perspectiveacma2010Nessuna valutazione finora
- Changing The Work Environment inDocumento8 pagineChanging The Work Environment inKassiani LavidaNessuna valutazione finora
- Cbabddd 273 B 3 A 6 e 024 e 5Documento8 pagineCbabddd 273 B 3 A 6 e 024 e 5api-620025002Nessuna valutazione finora
- IdentidadDocumento12 pagineIdentidadEdgarsito AyalaNessuna valutazione finora
- Theoretical Framework: A Model For Cancer CareDocumento3 pagineTheoretical Framework: A Model For Cancer CarevinothasoniNessuna valutazione finora
- Complex Care Management Toolkit PDFDocumento14 pagineComplex Care Management Toolkit PDFumi khasanahNessuna valutazione finora
- Kidney Careoutline1203Documento3 pagineKidney Careoutline1203weesiniNessuna valutazione finora
- IACSD 2020 GuidelinesDocumento122 pagineIACSD 2020 GuidelinesRicardo Del NiroNessuna valutazione finora
- Advanced Practice and Leadership in Radiology NursingDa EverandAdvanced Practice and Leadership in Radiology NursingKathleen A. GrossNessuna valutazione finora
- Challenges in Implementing Innovations in Midwifery Practice An OverviewDocumento3 pagineChallenges in Implementing Innovations in Midwifery Practice An OverviewEditor IJTSRDNessuna valutazione finora
- Development and Psychometric Testing of A CompeteDocumento6 pagineDevelopment and Psychometric Testing of A CompetethuongNessuna valutazione finora
- Osborne+et+al +the+health+education+impact+questionnaireDocumento10 pagineOsborne+et+al +the+health+education+impact+questionnairesandrine.abellarNessuna valutazione finora
- Professionalism in Nursing 6 - The Nurse As InnovatorDocumento4 pagineProfessionalism in Nursing 6 - The Nurse As InnovatorHana Lara LaitNessuna valutazione finora
- Clinical Research Associate - The Comprehensive Guide: Vanguard ProfessionalsDa EverandClinical Research Associate - The Comprehensive Guide: Vanguard ProfessionalsNessuna valutazione finora
- Providing Higher Value Care Through Population Health Management: What Is The Radiologist 'S Role?Documento2 pagineProviding Higher Value Care Through Population Health Management: What Is The Radiologist 'S Role?Camilo SotomayorNessuna valutazione finora
- Shadow ANurseDocumento8 pagineShadow ANurseSculpting FutureNessuna valutazione finora
- The Magic Programme EvaluationDocumento82 pagineThe Magic Programme EvaluationMihaela BerindeieNessuna valutazione finora
- 118 - Week 2Documento35 pagine118 - Week 2Ma. Kristina Cazandra IbañezNessuna valutazione finora
- Brewer 2015Documento6 pagineBrewer 2015Amelia WalimanNessuna valutazione finora
- Identifying Clinicians Priorities For The Implementation of Best Practices in Cognitive Rehabilitation Post Acquired Brain InjuryDocumento12 pagineIdentifying Clinicians Priorities For The Implementation of Best Practices in Cognitive Rehabilitation Post Acquired Brain Injuryu3505483Nessuna valutazione finora
- CF Exemplar NURS-FPX4020 Assessment 4Documento13 pagineCF Exemplar NURS-FPX4020 Assessment 4Sabahat BashirNessuna valutazione finora
- BSN IV e Group 1 Swot Analysis 1Documento52 pagineBSN IV e Group 1 Swot Analysis 13D - AURELIO, Lyca Mae M.Nessuna valutazione finora
- The Pivotal Role of Nursing PeDocumento8 pagineThe Pivotal Role of Nursing Pehisbullah alkhumaidiNessuna valutazione finora
- International Journal of Nursing StudiesDocumento12 pagineInternational Journal of Nursing StudiesraraNessuna valutazione finora
- Barriers, Facilitators, and ProposalsDocumento11 pagineBarriers, Facilitators, and ProposalsAisha MagarangNessuna valutazione finora
- 2013ISAlmost Correctionalnursing AstudyprotocoltodevelopaneducationalinterventionDocumento7 pagine2013ISAlmost Correctionalnursing AstudyprotocoltodevelopaneducationalinterventionAmeerah Mousa KhanNessuna valutazione finora
- Patient Safety: Paradigm Shift of Modern Healthcare Delivery and ResearchDocumento2 paginePatient Safety: Paradigm Shift of Modern Healthcare Delivery and ResearchInt J of Med Sci and Nurs ResNessuna valutazione finora
- The Clinician Role in Health Care Delivery and InnovationDocumento21 pagineThe Clinician Role in Health Care Delivery and InnovationLuis Henrique SalesNessuna valutazione finora
- Clinical quLITITYDocumento43 pagineClinical quLITITYppniNessuna valutazione finora
- Optimal EngDocumento11 pagineOptimal EngIRENE ORTIZ LOPEZNessuna valutazione finora
- INNOVATIONDocumento11 pagineINNOVATIONrajitha jayaprakashNessuna valutazione finora
- Qsen Research PaperDocumento5 pagineQsen Research Paperzijkchbkf100% (1)
- Workshop Materials BookletDocumento121 pagineWorkshop Materials BookletlyrechaugustNessuna valutazione finora
- Impact of Advanced Practice Nurses and Midwives On Patients' Outcomes: A Systematic ReviewDocumento6 pagineImpact of Advanced Practice Nurses and Midwives On Patients' Outcomes: A Systematic ReviewConsolata kirigiaNessuna valutazione finora
- Clinical Nursing JudgmentDocumento5 pagineClinical Nursing Judgmentapi-662884360Nessuna valutazione finora
- Using SBAR To Communicate Falls Risk and Management in Interprofessional Rehabilitation TeamsDocumento54 pagineUsing SBAR To Communicate Falls Risk and Management in Interprofessional Rehabilitation Teamsmehara1920Nessuna valutazione finora
- Using SBAR To Communicate Falls Risk and Management in Interprofessional Rehabilitation Teams PDFDocumento54 pagineUsing SBAR To Communicate Falls Risk and Management in Interprofessional Rehabilitation Teams PDFmehara1920Nessuna valutazione finora
- Conley - PGC ReflectionDocumento9 pagineConley - PGC Reflectionapi-458494853Nessuna valutazione finora
- Critical Thinking in Nursing Education: A Literature Review: CorrespondenceDocumento25 pagineCritical Thinking in Nursing Education: A Literature Review: CorrespondenceLheo AngelesNessuna valutazione finora
- Peer EducationDocumento8 paginePeer EducationEduarda DiasNessuna valutazione finora
- Producing Competent Physicians - More Paper Work or IndeedDocumento48 pagineProducing Competent Physicians - More Paper Work or Indeedapi-26176346Nessuna valutazione finora
- Interpersonal SkillsDocumento2 pagineInterpersonal SkillsUmarameshKNessuna valutazione finora
- Nursing Process Research PaperDocumento7 pagineNursing Process Research Paperafeawfxlb100% (1)
- Cahps Section 4 Ways To Approach Qi ProcessDocumento22 pagineCahps Section 4 Ways To Approach Qi ProcessojuNessuna valutazione finora
- Research in Continuing Education Programme: C. Meribha Christy, V. HemavathyDocumento4 pagineResearch in Continuing Education Programme: C. Meribha Christy, V. HemavathyRubina MasihNessuna valutazione finora
- JCI Whitepaper Cpgs Closing The GapDocumento12 pagineJCI Whitepaper Cpgs Closing The GapMathilda UllyNessuna valutazione finora
- Clinical Judgement PaperDocumento7 pagineClinical Judgement Paperapi-545666342Nessuna valutazione finora
- Clinical Nursing JudgmentDocumento8 pagineClinical Nursing Judgmentapi-402635887Nessuna valutazione finora
- Dissertation On Community Health NursingDocumento6 pagineDissertation On Community Health NursingBuyCollegePapersClearwater100% (1)
- Understanding The Patient Experience A ConceptualDocumento5 pagineUnderstanding The Patient Experience A ConceptualFrancisco BohorquezNessuna valutazione finora
- 2 PB PDFDocumento9 pagine2 PB PDFAnjeneth Bawit GumannaoNessuna valutazione finora
- Ijerph 18 02247 v2 1Documento24 pagineIjerph 18 02247 v2 1emmaNessuna valutazione finora
- Clinical Nursing JudgementDocumento6 pagineClinical Nursing Judgementapi-507960658Nessuna valutazione finora
- Assessment and Care Planning For Cancer Survivors Tcm9 297790Documento52 pagineAssessment and Care Planning For Cancer Survivors Tcm9 297790irinaelenamartiniucNessuna valutazione finora
- 14 Supporting Prevention and Chronic Condition Self-ManagementDocumento8 pagine14 Supporting Prevention and Chronic Condition Self-Managementilham apriadiNessuna valutazione finora
- 7 PDFDocumento7 pagine7 PDFStericho FerdinanNessuna valutazione finora
- Enhancing Clinical Practice in The Management of Distress: The Therapeutic Practices For Distress Management (TPDM) ProjectDocumento7 pagineEnhancing Clinical Practice in The Management of Distress: The Therapeutic Practices For Distress Management (TPDM) ProjectKarolinaMaślakNessuna valutazione finora
- Clinical Simulation: Changing The Landscape of Nursing EducationDocumento5 pagineClinical Simulation: Changing The Landscape of Nursing EducationKenneth Myro GarciaNessuna valutazione finora
- Contingency Management Approach: Implementation and OutcomesDocumento112 pagineContingency Management Approach: Implementation and OutcomesArun SharmaNessuna valutazione finora
- Case Demand Measurement and Forecasting Block-2 Ch.4Documento3 pagineCase Demand Measurement and Forecasting Block-2 Ch.4v_ratNessuna valutazione finora
- of E-Aushadi FinalDocumento48 pagineof E-Aushadi Finalv_ratNessuna valutazione finora
- Access To Quality Medicines: Rajasthan Model: "Reaching The Unreached"Documento7 pagineAccess To Quality Medicines: Rajasthan Model: "Reaching The Unreached"v_ratNessuna valutazione finora
- Marketing Research Chapter Case Block-2 Ch.5Documento4 pagineMarketing Research Chapter Case Block-2 Ch.5v_rat0% (1)
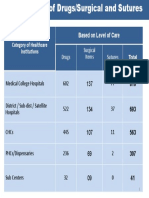
- Category of Healthcare Institutions Based On Level of Care: Drugs Surgical Items SuturesDocumento1 paginaCategory of Healthcare Institutions Based On Level of Care: Drugs Surgical Items Suturesv_ratNessuna valutazione finora
- Drugs Store Management: Dr. Nirmal GurbaniDocumento94 pagineDrugs Store Management: Dr. Nirmal Gurbaniv_ratNessuna valutazione finora
- Quantification of Health Commodities - RMNCH SupplementDocumento173 pagineQuantification of Health Commodities - RMNCH Supplementv_ratNessuna valutazione finora
- A Strategic Essential in Healthcare Systems OutsourcingDocumento22 pagineA Strategic Essential in Healthcare Systems Outsourcingv_ratNessuna valutazione finora
- Day 8 Inventory ManagementDocumento56 pagineDay 8 Inventory Managementv_ratNessuna valutazione finora
- UNFPA RFQ QA Framework - Low - V11Documento32 pagineUNFPA RFQ QA Framework - Low - V11v_ratNessuna valutazione finora
- Assessment of Patient Engagement With A Mobile Application Among Service Members in TransitionDocumento9 pagineAssessment of Patient Engagement With A Mobile Application Among Service Members in Transitionv_ratNessuna valutazione finora
- Inv. Mgt. Procurement & DistributionDocumento78 pagineInv. Mgt. Procurement & Distributionv_ratNessuna valutazione finora
- Day 4 - ReliabilityDocumento11 pagineDay 4 - Reliabilityv_ratNessuna valutazione finora
- Day 4 - CQI in Stores ManagementDocumento8 pagineDay 4 - CQI in Stores Managementv_ratNessuna valutazione finora
- Day 2 - Equipment Preventive MaintenanceDocumento29 pagineDay 2 - Equipment Preventive Maintenancev_ratNessuna valutazione finora
- Introduction To Epidemiology: Cohort StudiesDocumento32 pagineIntroduction To Epidemiology: Cohort Studiesv_ratNessuna valutazione finora
- Logistics Management Information Systems (LMIS)Documento25 pagineLogistics Management Information Systems (LMIS)v_ratNessuna valutazione finora
- Day 3 - Equipment Disposal, Audit, T&DDocumento35 pagineDay 3 - Equipment Disposal, Audit, T&Dv_ratNessuna valutazione finora
- Day 1 - Equipment-Mohan-1Documento22 pagineDay 1 - Equipment-Mohan-1v_ratNessuna valutazione finora
- The Case-Study Approach: Lucy GilsonDocumento74 pagineThe Case-Study Approach: Lucy Gilsonv_ratNessuna valutazione finora
- Patient Engagement Planning Checklist: Planning Component Key Questions To ConsiderDocumento2 paginePatient Engagement Planning Checklist: Planning Component Key Questions To Considerv_ratNessuna valutazione finora
- Patient Engagement in Research: A Systematic Review: Researcharticle Open AccessDocumento9 paginePatient Engagement in Research: A Systematic Review: Researcharticle Open Accessv_ratNessuna valutazione finora
- Health Affairs: For Reprints, Links & Permissions: E-Mail Alerts: To SubscribeDocumento9 pagineHealth Affairs: For Reprints, Links & Permissions: E-Mail Alerts: To Subscribev_ratNessuna valutazione finora
- Gulfpub Wo 201805Documento81 pagineGulfpub Wo 201805Patricia.PNessuna valutazione finora
- Solution Manual For C How To Program 8th Edition Paul J Deitel Harvey DeitelDocumento34 pagineSolution Manual For C How To Program 8th Edition Paul J Deitel Harvey Deiteldryas.czech0gkl100% (47)
- WB-Mech 120 Ch05 ModalDocumento16 pagineWB-Mech 120 Ch05 ModalhebiyongNessuna valutazione finora
- Qdoc - Tips Sinister-TarotzDocumento92 pagineQdoc - Tips Sinister-TarotzAleister DahmerNessuna valutazione finora
- Lesson 3: Letters of RequestDocumento4 pagineLesson 3: Letters of RequestMinh HiếuNessuna valutazione finora
- AWANA Handbook 2010-2011Documento8 pagineAWANA Handbook 2010-2011carriepratchard100% (1)
- MHD Exam 6 MaterialDocumento179 pagineMHD Exam 6 Materialnaexuis5467100% (1)
- Lean Six SigmaDocumento5 pagineLean Six SigmavinNessuna valutazione finora
- Debug and AssemblerDocumento9 pagineDebug and AssemblerManoj GurralaNessuna valutazione finora
- MP CRPDocumento2 pagineMP CRPankutupanaNessuna valutazione finora
- 2400 8560 PR 8010 - A1 HSE Management PlanDocumento34 pagine2400 8560 PR 8010 - A1 HSE Management PlanMohd Musa HashimNessuna valutazione finora
- Edagogy of Anguages: VerviewDocumento54 pagineEdagogy of Anguages: VerviewMukesh MalviyaNessuna valutazione finora
- PriceDoxy 09 September 2011Documento56 paginePriceDoxy 09 September 2011Elena OltuNessuna valutazione finora
- HimediaDocumento2 pagineHimediaWiwit MarianaNessuna valutazione finora
- Annex A2 - CS Form 100 - Revised 2023 - CSESP - A1 - Edited - A1Documento2 pagineAnnex A2 - CS Form 100 - Revised 2023 - CSESP - A1 - Edited - A1obs.obando2022Nessuna valutazione finora
- Unit 1 My Hobbies Lesson 1 Getting StartedDocumento14 pagineUnit 1 My Hobbies Lesson 1 Getting StartedhienNessuna valutazione finora
- Introduction To Entrepreneurship: Bruce R. Barringer R. Duane IrelandDocumento29 pagineIntroduction To Entrepreneurship: Bruce R. Barringer R. Duane IrelandAnonymous Yp8H9QwNessuna valutazione finora
- Water Quality MonitoringDocumento3 pagineWater Quality MonitoringJoa YupNessuna valutazione finora
- Applications Description: General Purpose NPN Transistor ArrayDocumento5 pagineApplications Description: General Purpose NPN Transistor ArraynudufoqiNessuna valutazione finora
- Study of Noise Mapping at Moolchand Road Phargang New DelhiDocumento10 pagineStudy of Noise Mapping at Moolchand Road Phargang New DelhiEditor IJTSRDNessuna valutazione finora
- Circuit Breaker - Ground & Test Device Type VR Electrically OperatedDocumento24 pagineCircuit Breaker - Ground & Test Device Type VR Electrically OperatedcadtilNessuna valutazione finora
- 311762en WDocumento36 pagine311762en WOprisor CostinNessuna valutazione finora
- Media Analysis-GraphicDocumento1 paginaMedia Analysis-Graphicapi-262266786100% (1)
- Cics 400 Administration and Operations GuideDocumento343 pagineCics 400 Administration and Operations GuidedafraumNessuna valutazione finora
- MC-8002 Mixer 2Documento1 paginaMC-8002 Mixer 2JAIDEV KUMAR RANINessuna valutazione finora
- Final Report of BBSMDocumento37 pagineFinal Report of BBSMraazoo1967% (9)
- A Review of Automatic License Plate Recognition System in Mobile-Based PlatformDocumento6 pagineA Review of Automatic License Plate Recognition System in Mobile-Based PlatformadiaNessuna valutazione finora
- Support of Roof and Side in Belowground Coal MinesDocumento5 pagineSupport of Roof and Side in Belowground Coal MinesNavdeep MandalNessuna valutazione finora
- Youth and Moral ValuesDocumento6 pagineYouth and Moral ValuesAlka SinghNessuna valutazione finora
- Lier Upper Secondary SchoolDocumento8 pagineLier Upper Secondary SchoolIES Río CabeNessuna valutazione finora