Potrebbero piacerti anche
- Textbook of Urgent Care Management: Chapter 35, Urgent Care Imaging and InterpretationDa EverandTextbook of Urgent Care Management: Chapter 35, Urgent Care Imaging and InterpretationNessuna valutazione finora
- Electronics 09 00121Documento15 pagineElectronics 09 00121praba821Nessuna valutazione finora
- 1998 A Software Package For Non-Invasive Real-Time Beat-To-Beat Monitoring of Stroke Volume PDFDocumento22 pagine1998 A Software Package For Non-Invasive Real-Time Beat-To-Beat Monitoring of Stroke Volume PDFDavid MadinaieNessuna valutazione finora
- Colorimeters Versus Spectrophotometers: Insight On ColorDocumento0 pagineColorimeters Versus Spectrophotometers: Insight On ColorGaurav AcharyaNessuna valutazione finora
- Computers in Biology and MedicineDocumento10 pagineComputers in Biology and Medicineisaí lozanoNessuna valutazione finora
- A Signal Processing Module For The Analysis of Heart Sounds and Heart MurmursDocumento9 pagineA Signal Processing Module For The Analysis of Heart Sounds and Heart MurmursAbdul SaboorNessuna valutazione finora
- Jec-Ecc 2016 7518962Documento4 pagineJec-Ecc 2016 7518962jesusNessuna valutazione finora
- Singh 2019Documento5 pagineSingh 2019Lakshmi ShettyNessuna valutazione finora
- Cardiac Magnetic Resonance Atlas: 101 Clinical CasesDa EverandCardiac Magnetic Resonance Atlas: 101 Clinical CasesNessuna valutazione finora
- 2020 IJ Scopus IJAST Divya LalithaDocumento10 pagine2020 IJ Scopus IJAST Divya LalithaR.V.S.LALITHANessuna valutazione finora
- 1 s2.0 S266709922200024X MainDocumento12 pagine1 s2.0 S266709922200024X MainBiomed BiomedNessuna valutazione finora
- David Et Al HeartrateDocumento5 pagineDavid Et Al HeartrateDae Hyun BaikNessuna valutazione finora
- Tach PaperDocumento9 pagineTach Papersarkodie kwameNessuna valutazione finora
- Jurnal 16 - An Internet-Based Tool For Pediatric Cardiac Disease Diagnosis Using Intelligent PhonocardiographyDocumento5 pagineJurnal 16 - An Internet-Based Tool For Pediatric Cardiac Disease Diagnosis Using Intelligent PhonocardiographyAngela Erti Suci RosariNessuna valutazione finora
- Computed-Tomography a Powerful Tool for Diagnosis of Pediatric and Adult Congenital Heart Disease: Methodology and Interpretation GuideDa EverandComputed-Tomography a Powerful Tool for Diagnosis of Pediatric and Adult Congenital Heart Disease: Methodology and Interpretation GuideNessuna valutazione finora
- Journal Pre-Proof: Computer Methods and Programs in BiomedicineDocumento23 pagineJournal Pre-Proof: Computer Methods and Programs in Biomedicinepuneet5246Nessuna valutazione finora
- Remotesensing 12 01685 With Cover PDFDocumento15 pagineRemotesensing 12 01685 With Cover PDFSusana MalleaNessuna valutazione finora
- Diagnostic Stethoscope Project SynopsisDocumento6 pagineDiagnostic Stethoscope Project SynopsisBhanu Pratap ReddyNessuna valutazione finora
- Biomedical Signal Processing and ApplicationsDocumento6 pagineBiomedical Signal Processing and ApplicationssreehariNessuna valutazione finora
- An Innovative Device For TMJ Vibration AnalysisDocumento7 pagineAn Innovative Device For TMJ Vibration AnalysisIJAR JOURNALNessuna valutazione finora
- R-HRV: An R-Based Software Package For Heart Rate Variability Analysis of ECG RecordingsDocumento9 pagineR-HRV: An R-Based Software Package For Heart Rate Variability Analysis of ECG RecordingsFiras ZakNessuna valutazione finora
- Medical Physics - 2021 - Praagh - Fully Automated Quantification Method FQM of Coronary Calcium in An AnthropomorphicDocumento12 pagineMedical Physics - 2021 - Praagh - Fully Automated Quantification Method FQM of Coronary Calcium in An AnthropomorphicAmril MukminNessuna valutazione finora
- 03 Performance Comparison of 6 In-Hospital Patient Monitoring Systems in The Detection and Alarm of Ventricular Cardiac ArrhythmiasDocumento8 pagine03 Performance Comparison of 6 In-Hospital Patient Monitoring Systems in The Detection and Alarm of Ventricular Cardiac ArrhythmiasxiaoxcorazonNessuna valutazione finora
- Goodfellow 18 ADocumento18 pagineGoodfellow 18 AMhd rdbNessuna valutazione finora
- A Configuration Smart Health Care Box For Medical ApplicationDocumento6 pagineA Configuration Smart Health Care Box For Medical ApplicationJREAS JOURNALNessuna valutazione finora
- Fin Irjmets1679911272Documento6 pagineFin Irjmets1679911272Kishore Kanna Ravi KumarNessuna valutazione finora
- BIOEN 481 Stethoscope Testing ReportDocumento7 pagineBIOEN 481 Stethoscope Testing ReportchaocharliehuangNessuna valutazione finora
- AsilomarPublication DigitalStethoscopeDocumento5 pagineAsilomarPublication DigitalStethoscopeMatthewMcTNessuna valutazione finora
- Heart Sound Analysis and ClassificationDocumento8 pagineHeart Sound Analysis and ClassificationVishwanath ShervegarNessuna valutazione finora
- Heart Disease Prediction Using Machine Learning - 2018Documento8 pagineHeart Disease Prediction Using Machine Learning - 2018dr mbaluNessuna valutazione finora
- 07 Dr. S. AnithaDocumento9 pagine07 Dr. S. AnithaS. LAVANYANessuna valutazione finora
- Arrhythmia Detection - A Machine Learning BasedDocumento5 pagineArrhythmia Detection - A Machine Learning BasedRyan Azmi Zuhdi DamanikNessuna valutazione finora
- Wireless Heart Attack Detection SystemDocumento3 pagineWireless Heart Attack Detection SystemIJSTENessuna valutazione finora
- Development of A Low Cost Fetal Heart Sound MonitoDocumento10 pagineDevelopment of A Low Cost Fetal Heart Sound MonitoShravya MNessuna valutazione finora
- Heart Beat MonitoringDocumento5 pagineHeart Beat MonitoringVishnu Sadasivan100% (1)
- Basic Knowledge of Medical Imaging Informatics: Undergraduate Level and Level IDa EverandBasic Knowledge of Medical Imaging Informatics: Undergraduate Level and Level IPeter M. A. van OoijenNessuna valutazione finora
- Sensors 20 04139Documento15 pagineSensors 20 04139soo chiNessuna valutazione finora
- Analysis of Heart Sound and Murmurs For Cardiac DisorderDocumento13 pagineAnalysis of Heart Sound and Murmurs For Cardiac DisorderAnjali NagarNessuna valutazione finora
- Computational Framework For Heart Disease Prediction Using Deep Belief Neural Network With Fuzzy LogicDocumento9 pagineComputational Framework For Heart Disease Prediction Using Deep Belief Neural Network With Fuzzy LogicMahmood SyedNessuna valutazione finora
- Robust Classification of Cardiac Arrhythmia Using Machine LearningDocumento9 pagineRobust Classification of Cardiac Arrhythmia Using Machine LearningIJRASETPublicationsNessuna valutazione finora
- Wa0012.Documento6 pagineWa0012.23Riya Khot VcetNessuna valutazione finora
- (IJETA-V7I3P2) : Sai Sruthi Gadde, Venkata Dinesh Reddy KalliDocumento5 pagine(IJETA-V7I3P2) : Sai Sruthi Gadde, Venkata Dinesh Reddy KalliIJETA - EighthSenseGroupNessuna valutazione finora
- Appi - Ajp.2019.19020212.ds001 - Suplemento en LineaDocumento22 pagineAppi - Ajp.2019.19020212.ds001 - Suplemento en LineaYorcys GutiérrezNessuna valutazione finora
- Animal Monitoring SysytemDocumento5 pagineAnimal Monitoring SysytemericNessuna valutazione finora
- Real-Time Remote Monitoring Cardiac Patients at Distance: Openecg Workshop 2004, Berlin, GermanyDocumento3 pagineReal-Time Remote Monitoring Cardiac Patients at Distance: Openecg Workshop 2004, Berlin, GermanydawadhaliNessuna valutazione finora
- Recommendations For Ecg Acquisition Using BitalinoDocumento6 pagineRecommendations For Ecg Acquisition Using BitalinoValeria Ramirez MedinaNessuna valutazione finora
- A Survey On Heart Disease Prediction Using Various Machine Learning TechniquesDocumento5 pagineA Survey On Heart Disease Prediction Using Various Machine Learning TechniquesIJRASETPublicationsNessuna valutazione finora
- Veri ChipDocumento33 pagineVeri ChipPraseetha RaoNessuna valutazione finora
- Stress Detection Using Machine Learning and Deep LDocumento9 pagineStress Detection Using Machine Learning and Deep LKrishna KumarNessuna valutazione finora
- Iot: Heart Rate Monitoring Tool Using Android With Alert Messanger Telegram SystemDocumento7 pagineIot: Heart Rate Monitoring Tool Using Android With Alert Messanger Telegram Systemriki capoeiristaNessuna valutazione finora
- Heart Rate Monitoring System Using FingeDocumento4 pagineHeart Rate Monitoring System Using FingeAndreea Ilie100% (1)
- For The First Time, MR and PET Are One.: Local Contact Information in The USADocumento14 pagineFor The First Time, MR and PET Are One.: Local Contact Information in The USARoberto Arriagada TrincadoNessuna valutazione finora
- EvaluacionDocumento4 pagineEvaluacionJhan ZitoNessuna valutazione finora
- Occupational Exposure of Physical TherapistsDocumento8 pagineOccupational Exposure of Physical Therapistsfreon1999Nessuna valutazione finora
- Biomedical Time Series Processing and Analysis Methods - The Case of EMDDocumento21 pagineBiomedical Time Series Processing and Analysis Methods - The Case of EMDlucianbejanNessuna valutazione finora
- Paper 8663Documento4 paginePaper 8663IJARSCT JournalNessuna valutazione finora
- Biomedical Instrumentation NotesDocumento13 pagineBiomedical Instrumentation NotesashvathNessuna valutazione finora
- Remote Sensing: Classification of Arrhythmia by Using Deep Learning With 2-D ECG Spectral Image RepresentationDocumento14 pagineRemote Sensing: Classification of Arrhythmia by Using Deep Learning With 2-D ECG Spectral Image RepresentationBhargav KodaliNessuna valutazione finora
- Heart Disease Prediction Model: DissertationDocumento4 pagineHeart Disease Prediction Model: DissertationGaurav MehraNessuna valutazione finora
- Arif Sir Question - ch1Documento22 pagineArif Sir Question - ch1MEHEDI HASANNessuna valutazione finora
- Undergraduate-Prospectus SsuetDocumento141 pagineUndergraduate-Prospectus SsuetRuman AnwarNessuna valutazione finora
- Mainboard EAX64290501Documento22 pagineMainboard EAX64290501Uzziel Mague0% (1)
- Disk Speed Test ManualDocumento78 pagineDisk Speed Test ManualKarl Si AkoNessuna valutazione finora
- PHD Literature Review LengthDocumento7 paginePHD Literature Review Lengthea3vk50y100% (1)
- Formulary - Aerodynamic Design of Turbomachinery: PV NRT, H HDocumento2 pagineFormulary - Aerodynamic Design of Turbomachinery: PV NRT, H HZhifengNessuna valutazione finora
- Probability of Bit Error For BPSK Modulation in An Awgn ChannelDocumento15 pagineProbability of Bit Error For BPSK Modulation in An Awgn Channel210ec3288Nessuna valutazione finora
- Introduction To HazidDocumento29 pagineIntroduction To Hazidafan nur arifNessuna valutazione finora
- How To Import Satellite Image From Google Earth To ArcGISDocumento10 pagineHow To Import Satellite Image From Google Earth To ArcGISMehmood AlamNessuna valutazione finora
- Resignation LetterDocumento1 paginaResignation LetterSaty AnandNessuna valutazione finora
- Precalculus Note Sequence SeriesDocumento4 paginePrecalculus Note Sequence Series01bourgeoisie 040104Nessuna valutazione finora
- ApplicationDocumento23 pagineApplicationGreen développementNessuna valutazione finora
- FA Annual Report 2021Documento28 pagineFA Annual Report 2021Charmaine SebastianNessuna valutazione finora
- 5-Digit Number Challenges 1: Use The Digits 3, 1, 2, 6, 9 To Make A 5-Digit Number Each TimeDocumento2 pagine5-Digit Number Challenges 1: Use The Digits 3, 1, 2, 6, 9 To Make A 5-Digit Number Each Timemarycperez0% (1)
- Model 115-3: Digital Electronic Control ValveDocumento36 pagineModel 115-3: Digital Electronic Control ValveBruno GonçalvesNessuna valutazione finora
- Soal PAT BING PG 30 SMT 1Documento11 pagineSoal PAT BING PG 30 SMT 1Laila FazaNessuna valutazione finora
- Samsung NP270E5E Lampard-AMD INT Rev 1.0 SchematicDocumento41 pagineSamsung NP270E5E Lampard-AMD INT Rev 1.0 SchematicAndré Frota Paiva100% (1)
- Blackweb BWA18AA010 - User ManualDocumento2 pagineBlackweb BWA18AA010 - User ManualAlejandro Manuel Collantes AlvarezNessuna valutazione finora
- UntitledDocumento16 pagineUntitledEmmanuel Doroteo NuñezNessuna valutazione finora
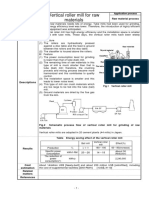
- Vertical Roller Mill For Raw MaterialsDocumento1 paginaVertical Roller Mill For Raw Materialsअहा मधुमक्खीपालनNessuna valutazione finora
- Kennvood DMF9020 SMDocumento29 pagineKennvood DMF9020 SMbetmenn45Nessuna valutazione finora
- Web result with site links: ఈనాడు: Telugu News - Latest Telugu News - Breaking ..Documento3 pagineWeb result with site links: ఈనాడు: Telugu News - Latest Telugu News - Breaking ..VamsiNessuna valutazione finora
- OCI Architect Associate (1Z0-1072)Documento52 pagineOCI Architect Associate (1Z0-1072)ikrudisNessuna valutazione finora
- 04 JP - WeldingDocumento8 pagine04 JP - WeldingShubhamShuklaNessuna valutazione finora
- ESP V-Programming & Data StructureDocumento70 pagineESP V-Programming & Data StructureAhana MukherjeeNessuna valutazione finora
- Global Vacuum Pressure Impregnation InsulationDocumento7 pagineGlobal Vacuum Pressure Impregnation InsulationanasawaisNessuna valutazione finora
- We're Programming Your Future: Melsec MedocDocumento8 pagineWe're Programming Your Future: Melsec MedocSlawaNessuna valutazione finora
- MA National Grid Utility BillDocumento2 pagineMA National Grid Utility Billjjtoomuch1118100% (2)
- Variable Voltaje AlternadorDocumento37 pagineVariable Voltaje AlternadorFrank Araya DiazNessuna valutazione finora
- Cambridge O Level: Second Language Urdu 3248/01Documento8 pagineCambridge O Level: Second Language Urdu 3248/01cima2k15Nessuna valutazione finora
- Home Theater LG DH4220S C/ DVD Player 330W RMS - 5.1 Canais, Conexão HDMI e USB, KaraokêDocumento1 paginaHome Theater LG DH4220S C/ DVD Player 330W RMS - 5.1 Canais, Conexão HDMI e USB, KaraokêTiara RoweNessuna valutazione finora