Potrebbero piacerti anche
- Design Basics: For Air and Surface DisinfectionDocumento10 pagineDesign Basics: For Air and Surface DisinfectionbarelihbNessuna valutazione finora
- Building and Environment: Minki Sung, Shinsuke KatoDocumento7 pagineBuilding and Environment: Minki Sung, Shinsuke KatoImran AzizNessuna valutazione finora
- Applications of Ultraviolet Germicidal Irradiation Disinfection in Health Care Facilities: Effective Adjunct, But Not Stand-Alone TechnologyDocumento12 pagineApplications of Ultraviolet Germicidal Irradiation Disinfection in Health Care Facilities: Effective Adjunct, But Not Stand-Alone TechnologyDavid Adolfo Paez MolinaNessuna valutazione finora
- UntitledDocumento25 pagineUntitledomar ahmedNessuna valutazione finora
- UVGI ApplicationDocumento12 pagineUVGI Applicationsakchai2012Nessuna valutazione finora
- Inactivation of Airborne Microorganisms Using Novel Ultraviolet Radiation Sources in Reflective Flow Through Control DevicesDocumento11 pagineInactivation of Airborne Microorganisms Using Novel Ultraviolet Radiation Sources in Reflective Flow Through Control DevicesMeduNessuna valutazione finora
- Artigo HarvardDocumento8 pagineArtigo HarvardDiego MatosNessuna valutazione finora
- ESTUDO Upper-Room Ultraviolet Light and Negative Air Ionization To Prevent Tuberculosis TransmissionDocumento12 pagineESTUDO Upper-Room Ultraviolet Light and Negative Air Ionization To Prevent Tuberculosis TransmissionClaudio SollarenNessuna valutazione finora
- Applications of Ultraviolet Germicidal Irradiation Disinfection in Health Care Facilities - Effective Adjunct, But Not Stand-Alone TechnologyDocumento12 pagineApplications of Ultraviolet Germicidal Irradiation Disinfection in Health Care Facilities - Effective Adjunct, But Not Stand-Alone TechnologyMichael LagundinoNessuna valutazione finora
- UV Data SheetDocumento9 pagineUV Data SheetArifin R HidayatNessuna valutazione finora
- Germicidal UV-C Disinfecting Air and Surfaces For DecadesDocumento8 pagineGermicidal UV-C Disinfecting Air and Surfaces For DecadesleandroniedbalskiNessuna valutazione finora
- 1 s2.0 S0195670123000609 MainDocumento9 pagine1 s2.0 S0195670123000609 MainAji DharmawanNessuna valutazione finora
- L5 Reducerea încӑrcӑturii microbiene a produselor alimentare folosind pulsuri de radiație UVDocumento8 pagineL5 Reducerea încӑrcӑturii microbiene a produselor alimentare folosind pulsuri de radiație UVOpreaNessuna valutazione finora
- View PDFDocumento14 pagineView PDFChandan MNessuna valutazione finora
- UV Disinfection of N95 Filtering Facepiece Respirators: A Brief ReviewDocumento9 pagineUV Disinfection of N95 Filtering Facepiece Respirators: A Brief ReviewNory González RomeroNessuna valutazione finora
- New UV Light Lamp To Fight Spread of InfluenzaDocumento3 pagineNew UV Light Lamp To Fight Spread of InfluenzaDan BosakNessuna valutazione finora
- Research of William Wells at HarvardDocumento10 pagineResearch of William Wells at HarvardARGHA MANNANessuna valutazione finora
- UV Sterilization of Personal Protective Equipment With Idle Laboratory Biosafety Cabinets During The COVID-19 PandemicDocumento13 pagineUV Sterilization of Personal Protective Equipment With Idle Laboratory Biosafety Cabinets During The COVID-19 PandemicNene SalazarNessuna valutazione finora
- IUVA Fact Sheet On COVID-19Documento3 pagineIUVA Fact Sheet On COVID-19Karen Pemintel LiadoNessuna valutazione finora
- Nardel Luz UV en Refugios Estudio de Seguridad 2008Documento9 pagineNardel Luz UV en Refugios Estudio de Seguridad 2008Vigilancia EpidemiologicaNessuna valutazione finora
- Applications of Ultraviolet Germicidal Irradiation Disinfection in Health Care FacilitiesDocumento13 pagineApplications of Ultraviolet Germicidal Irradiation Disinfection in Health Care FacilitiesJoao SousaNessuna valutazione finora
- Journal Pre-Proof: Journal of The American Academy of DermatologyDocumento9 pagineJournal Pre-Proof: Journal of The American Academy of DermatologyRajesh DeshmukhNessuna valutazione finora
- Catalogue Kover SRL En.Documento32 pagineCatalogue Kover SRL En.Ali Ben HusseinNessuna valutazione finora
- Hpac Magazine-Reviewing Iaq Best Practices For Building Engineers-April 2021Documento9 pagineHpac Magazine-Reviewing Iaq Best Practices For Building Engineers-April 2021api-328841994Nessuna valutazione finora
- UV Sterilization of Personal Protective Equipment With Idle Laboratory Biosafety Cabinets During The COVID-19 PandemicDocumento13 pagineUV Sterilization of Personal Protective Equipment With Idle Laboratory Biosafety Cabinets During The COVID-19 PandemicrickyNessuna valutazione finora
- Wang Et Al., 2019Documento9 pagineWang Et Al., 2019Bianca MariseNessuna valutazione finora
- Experimental Investigation of Indoor Aerosol Dispersion and Accumulation in The Context of COVID-19: Effects of Masks and VentilationDocumento14 pagineExperimental Investigation of Indoor Aerosol Dispersion and Accumulation in The Context of COVID-19: Effects of Masks and VentilationDaniel CarvajalNessuna valutazione finora
- Art 1Documento11 pagineArt 1Priscilla Bandeira FrotaNessuna valutazione finora
- Apm2011 124064Documento22 pagineApm2011 124064MeyshiaNessuna valutazione finora
- Hart2018. UV Radiation-Induced ImmunosuppressionDocumento13 pagineHart2018. UV Radiation-Induced Immunosuppressioncristina.moya724Nessuna valutazione finora
- Accepted Manuscript: It Is Time To Address Airborne Transmission of COVID-19Documento9 pagineAccepted Manuscript: It Is Time To Address Airborne Transmission of COVID-19Anonymous 9wHscMNessuna valutazione finora
- WeberDocumento13 pagineWeberachrafkchaw96888939Nessuna valutazione finora
- How To Reduce Airborne Pathogens Using Germicidal TechnologyDocumento8 pagineHow To Reduce Airborne Pathogens Using Germicidal TechnologyJUANNessuna valutazione finora
- Research On Effect of UV C Light On Bacteria and VirusesDocumento5 pagineResearch On Effect of UV C Light On Bacteria and VirusesEditor IJTSRDNessuna valutazione finora
- UV Data SheetDocumento15 pagineUV Data SheetBrian ThompsonNessuna valutazione finora
- UVGI Design Basics For Air and Surface Disinfection: January 2000Documento11 pagineUVGI Design Basics For Air and Surface Disinfection: January 2000Miguel FloresNessuna valutazione finora
- Survival of Bacteria On Respirator FiltersDocumento10 pagineSurvival of Bacteria On Respirator Filtersana carolina PereiraNessuna valutazione finora
- Airborne Bacterial Dispersal During and After Dressing and Bed Changes On Burns PatientsDocumento10 pagineAirborne Bacterial Dispersal During and After Dressing and Bed Changes On Burns Patientsicehorizon88Nessuna valutazione finora
- Referência 5Documento12 pagineReferência 5jmaj jmajNessuna valutazione finora
- UVGI Design Basics For Air and Surface Disinfection: January 2000Documento11 pagineUVGI Design Basics For Air and Surface Disinfection: January 2000Engr. MohidNessuna valutazione finora
- UV Disinfection of Water The Need For UV Reactor ValidationDocumento8 pagineUV Disinfection of Water The Need For UV Reactor ValidationMohammadreza NaghaviNessuna valutazione finora
- English TextDocumento2 pagineEnglish Textfmontaner1Nessuna valutazione finora
- Sanuvox Case StudiesDocumento4 pagineSanuvox Case StudiesMohd Khairunie IhsanNessuna valutazione finora
- UVGI Design Basics PDFDocumento10 pagineUVGI Design Basics PDFMeduNessuna valutazione finora
- Ou 2021 Jpn. J. Appl. Phys. 60 100501Documento8 pagineOu 2021 Jpn. J. Appl. Phys. 60 100501ventasNessuna valutazione finora
- Application Guide: Solution Air-Handling Units Uv-C Light OptionsDocumento12 pagineApplication Guide: Solution Air-Handling Units Uv-C Light OptionsBruno GuedesNessuna valutazione finora
- UV Data SheetDocumento12 pagineUV Data SheetvermdocamitNessuna valutazione finora
- Containment of Procedure-Associated Aerosols by An Extractor Tent: Effect On Nebulized Drug Particle DispersalDocumento6 pagineContainment of Procedure-Associated Aerosols by An Extractor Tent: Effect On Nebulized Drug Particle DispersalRSH Galaxy rehab medikNessuna valutazione finora
- Planning of Single-Used Mask Waste Containers As Personal Protective Equipment: A Case Study of Jakarta City StationDocumento8 paginePlanning of Single-Used Mask Waste Containers As Personal Protective Equipment: A Case Study of Jakarta City StationIJPHSNessuna valutazione finora
- UVR Whitepaper6 Airstream InDuct Disinfection 90000630 REV A 083120Documento4 pagineUVR Whitepaper6 Airstream InDuct Disinfection 90000630 REV A 083120JUANNessuna valutazione finora
- Far-UVC Light (222 NM) Efficiently and Safely Inactivates Airborne Human CoronavirusesDocumento8 pagineFar-UVC Light (222 NM) Efficiently and Safely Inactivates Airborne Human Coronaviruses王子瑜Nessuna valutazione finora
- Case Study 2Documento5 pagineCase Study 2Sanjeev KushwahaNessuna valutazione finora
- Detection of Viruses in Used Ventilation Filters From Two Large Public BuildingsDocumento9 pagineDetection of Viruses in Used Ventilation Filters From Two Large Public BuildingsbaridinoNessuna valutazione finora
- Science Abg2025Documento4 pagineScience Abg2025asdfNessuna valutazione finora
- Technological Institute of The Philippines: Department of Chemical EngineeringDocumento2 pagineTechnological Institute of The Philippines: Department of Chemical EngineeringRojen YuriNessuna valutazione finora
- Technological Institute of The Philippines: Department of Chemical EngineeringDocumento2 pagineTechnological Institute of The Philippines: Department of Chemical EngineeringRojen YuriNessuna valutazione finora
- Conditioning Systems: Effect On Office Worker Germicidal Ultraviolet Irradiation in AirDocumento7 pagineConditioning Systems: Effect On Office Worker Germicidal Ultraviolet Irradiation in Airjames2343eeNessuna valutazione finora
- Design and Fabrication of Portable PPE Kit SterilizationDocumento12 pagineDesign and Fabrication of Portable PPE Kit SterilizationIJRASETPublicationsNessuna valutazione finora
- Photochem Photobiol Publ +WSU 1-25-21Documento3 paginePhotochem Photobiol Publ +WSU 1-25-21Bill DavisNessuna valutazione finora
- Radiation Hormesis and the Linear-No-Threshold AssumptionDa EverandRadiation Hormesis and the Linear-No-Threshold AssumptionNessuna valutazione finora
- Low Temperature StorageDocumento2 pagineLow Temperature StorageIbnu HanafiNessuna valutazione finora
- BWT CatalogueDocumento2 pagineBWT CatalogueIbnu HanafiNessuna valutazione finora
- Low Temperature Storage Rev1Documento4 pagineLow Temperature Storage Rev1Ibnu HanafiNessuna valutazione finora
- Low Temp Pres - Kemenkes Vaksin Rev5Documento30 pagineLow Temp Pres - Kemenkes Vaksin Rev5Ibnu HanafiNessuna valutazione finora
- FORM Sponsorship Agreement (20 Feb)Documento4 pagineFORM Sponsorship Agreement (20 Feb)Ibnu HanafiNessuna valutazione finora
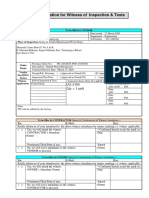
- MVAC Testing & Commissioning Procedure - 2007Documento245 pagineMVAC Testing & Commissioning Procedure - 2007spencersiu100% (6)
- TO PRINT 7AthSPONSORSHIP PROPOSAL - IEECCEDocumento30 pagineTO PRINT 7AthSPONSORSHIP PROPOSAL - IEECCEIbnu HanafiNessuna valutazione finora
- Chiller Vs VRFDocumento1 paginaChiller Vs VRFIbnu HanafiNessuna valutazione finora
- s71200 Easy Book en-US en-US PDFDocumento454 pagines71200 Easy Book en-US en-US PDFxendikaNessuna valutazione finora
- Form AFIDocumento1 paginaForm AFIIbnu HanafiNessuna valutazione finora
- Grundfosliterature 1073143 PDFDocumento48 pagineGrundfosliterature 1073143 PDFIbnu HanafiNessuna valutazione finora
- Attachment-4 - BQ & Information Required From Bidder - Rev B - MHE RevDocumento45 pagineAttachment-4 - BQ & Information Required From Bidder - Rev B - MHE RevIbnu HanafiNessuna valutazione finora
- Low Delta TDocumento4 pagineLow Delta TIbnu HanafiNessuna valutazione finora
- Basic Refrigeration 1Documento29 pagineBasic Refrigeration 1Ibnu HanafiNessuna valutazione finora
- Daikin Magnitude Magnetic Bearing ChillersDocumento27 pagineDaikin Magnitude Magnetic Bearing ChillersIbnu HanafiNessuna valutazione finora
- 01 Gi Industrial ASIA Holding WELCOME Distributors Meeting 20170718Documento7 pagine01 Gi Industrial ASIA Holding WELCOME Distributors Meeting 20170718Ibnu HanafiNessuna valutazione finora
- Final Oral Revalida Internal Medicine Compilation 1Documento45 pagineFinal Oral Revalida Internal Medicine Compilation 1Joel SaluNessuna valutazione finora
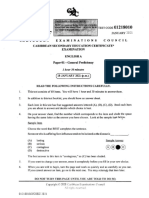
- CSEC English A January 2021 P1Documento16 pagineCSEC English A January 2021 P1Sasha FrostNessuna valutazione finora
- UntitledDocumento57 pagineUntitledAkram chaudaryNessuna valutazione finora
- Florida Task Force Report 9.1.20Documento14 pagineFlorida Task Force Report 9.1.20ABC Action NewsNessuna valutazione finora
- 12 Traumatic Conditions of The Lower Limb Final ?Documento52 pagine12 Traumatic Conditions of The Lower Limb Final ?Afaf Al Oufi AfafNessuna valutazione finora
- Hema 2 AssDocumento2 pagineHema 2 AssChatie PipitNessuna valutazione finora
- Ao 2012 0001Documento56 pagineAo 2012 0001Dennis FuentesNessuna valutazione finora
- Microbiology and ParasitologyDocumento53 pagineMicrobiology and ParasitologyJanlyn Ricci S. TañoNessuna valutazione finora
- AmenorrheaDocumento32 pagineAmenorrheaRajveerNessuna valutazione finora
- Trends in HIV Prevalence, Estimated HIV Incidence, and Risk Behavior Among Men Who Have Sex With Men in Bangkok, Thailand, 2003-2007Documento6 pagineTrends in HIV Prevalence, Estimated HIV Incidence, and Risk Behavior Among Men Who Have Sex With Men in Bangkok, Thailand, 2003-2007IietAyu05Nessuna valutazione finora
- Periorbital Edema: A Puzzle No More?: ReviewDocumento10 paginePeriorbital Edema: A Puzzle No More?: ReviewJavier Infantes MolinaNessuna valutazione finora
- Ijcmr 1538 3Documento8 pagineIjcmr 1538 3drelvNessuna valutazione finora
- Aspergillus Brasiliensis: (Atcc 16404™)Documento2 pagineAspergillus Brasiliensis: (Atcc 16404™)arsa1aNessuna valutazione finora
- Lymph FullDocumento4 pagineLymph Fullmayada elmakkiNessuna valutazione finora
- Non-Invasive Respiratory Support, Third Edition - Simonds, Anita K. (SRG) PDFDocumento385 pagineNon-Invasive Respiratory Support, Third Edition - Simonds, Anita K. (SRG) PDFCristinaLucanNessuna valutazione finora
- Finals MaternalDocumento30 pagineFinals MaternalPreciousmae Talay JavierNessuna valutazione finora
- Etiology of Epilepsy PDFDocumento2 pagineEtiology of Epilepsy PDFKellieNessuna valutazione finora
- Law Relating To HealthcareDocumento6 pagineLaw Relating To HealthcareSerena JamesNessuna valutazione finora
- Pain and Sensory DeprivationDocumento29 paginePain and Sensory DeprivationDivya sharma100% (1)
- Drains in SurgeryDocumento66 pagineDrains in SurgeryBalaji MallaNessuna valutazione finora
- Bosh So1 Training ModuleDocumento134 pagineBosh So1 Training ModuleRick Conley AdrielNessuna valutazione finora
- Nme 427 1meDocumento33 pagineNme 427 1meAriel Gamboa100% (1)
- Jurnal Dokter KeluargaDocumento7 pagineJurnal Dokter KeluargaJojo McalisterNessuna valutazione finora
- 1 Patient Assessment Form.Documento3 pagine1 Patient Assessment Form.Aina HaravataNessuna valutazione finora
- 3 IhDocumento42 pagine3 IhGennelyn Ross Delos ReyesNessuna valutazione finora
- Preparation of Organizational Chart of College and HospitalDocumento46 paginePreparation of Organizational Chart of College and HospitalJyothi RameshNessuna valutazione finora
- PSM Bhalani AnswerDocumento423 paginePSM Bhalani Answerpatilysh1100% (1)
- Semey State Medical University: Department of Psychiatry Topic Schizophrenia Raja Ali HassanDocumento45 pagineSemey State Medical University: Department of Psychiatry Topic Schizophrenia Raja Ali HassanRaja HassanNessuna valutazione finora
- The Pre-Tox Protocol How To Prepare Your Body For DetoxificationDocumento13 pagineThe Pre-Tox Protocol How To Prepare Your Body For DetoxificationSabrinaHaldemannNessuna valutazione finora