Potrebbero piacerti anche
- ICU ProtocolsDocumento35 pagineICU ProtocolsJohn Reynolds100% (6)
- Perioperative NursingDocumento24 paginePerioperative Nursingann aquino100% (1)
- Postoperative Fever - UpToDate PDFDocumento25 paginePostoperative Fever - UpToDate PDFkatsuiaNessuna valutazione finora
- PreOperative CareDocumento9 paginePreOperative CareYana Pot100% (2)
- To Be Submitted By: Ma. Therese P. Ballares BSN 2 - NCDocumento6 pagineTo Be Submitted By: Ma. Therese P. Ballares BSN 2 - NCMaria ThereseNessuna valutazione finora
- Perioperative LectureDocumento45 paginePerioperative LectureGaoudam NatarajanNessuna valutazione finora
- Perioperative NursingDocumento155 paginePerioperative NursingEissac100% (1)
- Tulio E. Bertorini - Neuromuscular DisordersDocumento466 pagineTulio E. Bertorini - Neuromuscular DisordersLeila Gonzalez100% (1)
- The Gunn Approach To The Treatment of Chronic PainDocumento185 pagineThe Gunn Approach To The Treatment of Chronic PainSamuelSeto75% (12)
- Perioperative Care For CABG PatientsDocumento32 paginePerioperative Care For CABG PatientsAya EyadNessuna valutazione finora
- OB Case StudyDocumento52 pagineOB Case StudyMaria ThereseNessuna valutazione finora
- Pulmonaryembolism 150329161109 Conversion Gate01Documento60 paginePulmonaryembolism 150329161109 Conversion Gate01Rafika RaraNessuna valutazione finora
- The Preoperative EvaluationDocumento25 pagineThe Preoperative Evaluationnormie littlemonsterNessuna valutazione finora
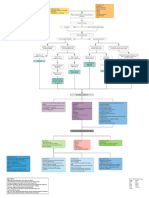
- Myocardial Infarction With CABG Concept MapDocumento1 paginaMyocardial Infarction With CABG Concept MapMaria Therese100% (1)
- Postpartum ComplicationsDocumento42 paginePostpartum ComplicationsElvisNessuna valutazione finora
- Bsn3-2c UC-BCF CVA Case StudyDocumento49 pagineBsn3-2c UC-BCF CVA Case StudyclarheenaNessuna valutazione finora
- Operating RoomDocumento81 pagineOperating Roomjaypee01100% (3)
- PeriopDocumento48 paginePeriopCherry Ann Garcia Durante100% (1)
- ICU AlgorithmsDocumento45 pagineICU AlgorithmsHashimIdreesNessuna valutazione finora
- Pedia Case StudyDocumento55 paginePedia Case StudyMaria Therese100% (1)
- FC Orth (SA) Intermediate Past Papers - 2012 Sept 28-3-2015Documento2 pagineFC Orth (SA) Intermediate Past Papers - 2012 Sept 28-3-2015Uhuebor DavidNessuna valutazione finora
- Operating Room Nursing: Vergel G. Leonardo Rn. ManDocumento72 pagineOperating Room Nursing: Vergel G. Leonardo Rn. ManRalph Lorenz Avila AquinoNessuna valutazione finora
- Candidate 219 DR Sangeetha Pai-My FRCS Experience PDFDocumento10 pagineCandidate 219 DR Sangeetha Pai-My FRCS Experience PDFBintealiNessuna valutazione finora
- 2006, Vol.24, Issues 1, Brain Injury and Cardiac ArrestDocumento169 pagine2006, Vol.24, Issues 1, Brain Injury and Cardiac ArrestKishore Reddy BhavanamNessuna valutazione finora
- Coventry 06.2012Documento14 pagineCoventry 06.2012karan270Nessuna valutazione finora
- Medical and Surgical Study Guide: by April Mae LabradorDocumento16 pagineMedical and Surgical Study Guide: by April Mae LabradorRalph Lorenz Avila AquinoNessuna valutazione finora
- Ati Med SurgDocumento36 pagineAti Med SurgVanessaMUeller94% (17)
- Critical Care Handbook 2013 PDFDocumento118 pagineCritical Care Handbook 2013 PDFpracesar3871Nessuna valutazione finora
- Case Analysis: Pre-OperativeDocumento12 pagineCase Analysis: Pre-OperativeMaria ThereseNessuna valutazione finora
- Acute Ischaemic StrokeDocumento40 pagineAcute Ischaemic StrokeDana Crusoveanu100% (1)
- Perawatan Perioperatif 1Documento72 paginePerawatan Perioperatif 1Jesika VitamaniaNessuna valutazione finora
- Practice Teaching On Pre and Post Op Nursing Care of Neurosurgery PatientsDocumento15 paginePractice Teaching On Pre and Post Op Nursing Care of Neurosurgery PatientsPriya SinghNessuna valutazione finora
- December 2008final FRCA VivaDocumento43 pagineDecember 2008final FRCA Vivajahangirealam100% (2)
- Complications of FractureDocumento19 pagineComplications of FractureEsome Sharma100% (1)
- Perioperative NursingDocumento11 paginePerioperative NursingMary Rias80% (5)
- CPG 2013 - Prevention and Treatment of Venous ThromboembolismDocumento170 pagineCPG 2013 - Prevention and Treatment of Venous ThromboembolismMia Mus100% (1)
- Monitoring & Devices Used in ICU CCUDocumento48 pagineMonitoring & Devices Used in ICU CCUProf. Ramsharan MehtaNessuna valutazione finora
- Deep Vein ThrombosisDocumento196 pagineDeep Vein ThrombosisCismaru Mirela Veronica0% (1)
- MainOR SyllabusDocumento208 pagineMainOR Syllabuster100% (1)
- Caz Clinic ORL PDFDocumento7 pagineCaz Clinic ORL PDFNorbert StenczelNessuna valutazione finora
- Case Study On Head InjuryDocumento15 pagineCase Study On Head InjuryPriya SinghNessuna valutazione finora
- 4 Mathers2012Documento5 pagine4 Mathers2012abdeali hazariNessuna valutazione finora
- Medical Surgical ReviewerDocumento9 pagineMedical Surgical ReviewerMary Ann Sambo OgoyNessuna valutazione finora
- Heart Failure (Congestive Heart Failure) FINALDocumento6 pagineHeart Failure (Congestive Heart Failure) FINALKristian Karl Bautista Kiw-isNessuna valutazione finora
- Choque MedularDocumento77 pagineChoque MedularEva Yazmin Perez MartinezNessuna valutazione finora
- Final MO Handbook 200510Documento171 pagineFinal MO Handbook 200510dreamyirisNessuna valutazione finora
- Gnur 405 SuzyDocumento6 pagineGnur 405 SuzySeth MensahNessuna valutazione finora
- CC Open Heart PaperDocumento5 pagineCC Open Heart Paperapi-738765099Nessuna valutazione finora
- DeliriumDocumento4 pagineDeliriumkotamalathi63Nessuna valutazione finora
- Project Yogi 3Documento141 pagineProject Yogi 3Mukesh kannan MahiNessuna valutazione finora
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Documento24 pagineP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)hendra2darmawanNessuna valutazione finora
- Med Surg Concept Map Clinical Make UpDocumento6 pagineMed Surg Concept Map Clinical Make UpColin MillerNessuna valutazione finora
- Thall PresentationDocumento27 pagineThall Presentationapi-211063572Nessuna valutazione finora
- CarbuncleDocumento14 pagineCarbuncleMohd Anuar IbrahimNessuna valutazione finora
- NCM 112 Perioperative ReviewerDocumento18 pagineNCM 112 Perioperative RevieweriamunknownnnnnnnNessuna valutazione finora
- Mangaoang Assignment in NCM 116 LEC Perception and CoordinationDocumento12 pagineMangaoang Assignment in NCM 116 LEC Perception and CoordinationDeinielle Magdangal RomeroNessuna valutazione finora
- Fundamental of Nursing 3Documento7 pagineFundamental of Nursing 3Atom AtomicNessuna valutazione finora
- TRIGGER 1: Preparing The Patient For Theatre Nutrition and HydrationDocumento3 pagineTRIGGER 1: Preparing The Patient For Theatre Nutrition and HydrationviolilahNessuna valutazione finora
- Ch. 18 Preoperative Nursing ManagementDocumento11 pagineCh. 18 Preoperative Nursing Managementth233Nessuna valutazione finora
- Consensus Statement On Brain Death - Malaysia - 2003Documento25 pagineConsensus Statement On Brain Death - Malaysia - 2003docpunit100% (1)
- Acute Myocardial Infarction (AMI)Documento92 pagineAcute Myocardial Infarction (AMI)Melissa SalayogNessuna valutazione finora
- Perioperative IIDocumento10 paginePerioperative IIshaghafalaghparyNessuna valutazione finora
- Material paraDocumento89 pagineMaterial pararoberto gomesNessuna valutazione finora
- Renal Transplant ThesisDocumento8 pagineRenal Transplant Thesisicatryhig100% (2)
- Health Teaching On Ta - HbsoDocumento3 pagineHealth Teaching On Ta - Hbsomecz26Nessuna valutazione finora
- Ramos PS ACTIVITY2 WEEK5Documento12 pagineRamos PS ACTIVITY2 WEEK5Jamaica Leslie NovenoNessuna valutazione finora
- Spinal Cord CompressionDocumento57 pagineSpinal Cord CompressionSherilNessuna valutazione finora
- Lecture 23Documento28 pagineLecture 23Danica PelegrinoNessuna valutazione finora
- Perioperative Care For Kidney Patients: KeywordsDocumento6 paginePerioperative Care For Kidney Patients: KeywordsAziil LiizaNessuna valutazione finora
- Sample of Medical and Surirgical NursingDocumento8 pagineSample of Medical and Surirgical NursingMounir ChadliNessuna valutazione finora
- PMLS 1 Module 2Documento7 paginePMLS 1 Module 2Jayson B. SanchezNessuna valutazione finora
- Persiapan Pra Operasi: Bagian/ SMF Anestesiologi Rs Islam Sultan Agung/ Fakultas Kedokteran Unissula 2007Documento22 paginePersiapan Pra Operasi: Bagian/ SMF Anestesiologi Rs Islam Sultan Agung/ Fakultas Kedokteran Unissula 2007ariahenkusNessuna valutazione finora
- Pre Op SyllabusDocumento50 paginePre Op Syllabusmunira.2707Nessuna valutazione finora
- Lectures in Neurosurgery For Medical Students.Documento87 pagineLectures in Neurosurgery For Medical Students.Tej Thatthi100% (1)
- Case Analysis: Medical Surgical NursingDocumento7 pagineCase Analysis: Medical Surgical NursingMaria ThereseNessuna valutazione finora
- PBL DiscussionsDocumento70 paginePBL DiscussionsMaria ThereseNessuna valutazione finora
- Case Study: Ethical DilemmaDocumento2 pagineCase Study: Ethical DilemmaMaria ThereseNessuna valutazione finora
- Growing FetusDocumento4 pagineGrowing FetusMaria ThereseNessuna valutazione finora
- Brain Drain Concept PaperDocumento4 pagineBrain Drain Concept PaperMaria ThereseNessuna valutazione finora
- Nursing Care Plan #1: IndependentDocumento3 pagineNursing Care Plan #1: IndependentMaria ThereseNessuna valutazione finora
- MalariaDocumento7 pagineMalariaMaria ThereseNessuna valutazione finora
- Malnutrition NCPDocumento1 paginaMalnutrition NCPMaria Therese100% (1)
- Ehealth ReportDocumento6 pagineEhealth ReportMaria ThereseNessuna valutazione finora
- Physical AssessmentDocumento14 paginePhysical AssessmentMaria ThereseNessuna valutazione finora
- Physical AssessmentDocumento37 paginePhysical AssessmentMaria ThereseNessuna valutazione finora
- Gyne Case StudyDocumento46 pagineGyne Case StudyMaria Therese100% (1)
- LEC Gallery WalkDocumento1 paginaLEC Gallery WalkMaria ThereseNessuna valutazione finora
- Adequacy of Scrubbing, Gowning and Gloving Among Operating Room NursesDocumento4 pagineAdequacy of Scrubbing, Gowning and Gloving Among Operating Room NursesMaria ThereseNessuna valutazione finora
- LEC ArticleDocumento2 pagineLEC ArticleMaria ThereseNessuna valutazione finora
- Modalities & Wound CareDocumento0 pagineModalities & Wound CareAndika Laksmana KurniadiNessuna valutazione finora
- StreptokinaseDocumento5 pagineStreptokinaseAnjali SinghNessuna valutazione finora
- Total Hip and Total Knee Replacement Post Operatif Nursing ManagementDocumento5 pagineTotal Hip and Total Knee Replacement Post Operatif Nursing ManagementAnas KhafidNessuna valutazione finora
- 5 Deep Vein Thrombosis Nursing Care PlansDocumento7 pagine5 Deep Vein Thrombosis Nursing Care PlansSubhranil MaityNessuna valutazione finora
- Deep Vein ThrombosisDocumento10 pagineDeep Vein Thrombosisزيد مسعودNessuna valutazione finora
- A History of Pulmonary Embolism and Deep Venous ThrombosisDocumento17 pagineA History of Pulmonary Embolism and Deep Venous ThrombosisAleksVaReNessuna valutazione finora
- Effects of Endotoxin On Pacemaker Funny Current in Hek 293 CellsDocumento190 pagineEffects of Endotoxin On Pacemaker Funny Current in Hek 293 CellsNemo SecretNessuna valutazione finora
- Role of DOAC in The Management of COVID-19 Patients: Desak Nyoman Desy LestariDocumento32 pagineRole of DOAC in The Management of COVID-19 Patients: Desak Nyoman Desy Lestaridesy lestariNessuna valutazione finora
- Deep Vein ThrombosisDocumento4 pagineDeep Vein ThrombosisAgatha FeliciaNessuna valutazione finora
- Pelvis: Stable Pelvic FracturesDocumento4 paginePelvis: Stable Pelvic FracturesEloise PateñoNessuna valutazione finora
- Managing Pulmonary EmbolismDocumento9 pagineManaging Pulmonary EmbolismTahaNessuna valutazione finora
- Puerperal SepsisDocumento30 paginePuerperal Sepsisjonaa2564Nessuna valutazione finora
- Air TravelDocumento6 pagineAir TravelGulfishan HaqNessuna valutazione finora
- Prev and Therapy For DVT. Dr. Suega SP - PDDocumento27 paginePrev and Therapy For DVT. Dr. Suega SP - PDAndre F SusantioNessuna valutazione finora
- DVTDocumento7 pagineDVTAnggun SafariantiniNessuna valutazione finora
- Pulmonary Embolism: Amina Adel Al-QaysiDocumento37 paginePulmonary Embolism: Amina Adel Al-QaysiJasleen Kaur100% (2)
- Xarelto Tablet Salut Selaput 20 MG - Rivaroksaban - DKI1251602517C1 - 2020Documento26 pagineXarelto Tablet Salut Selaput 20 MG - Rivaroksaban - DKI1251602517C1 - 2020Dimas RfNessuna valutazione finora
- Materi Keselamatan Dan Kesehatan PenerbanganDocumento16 pagineMateri Keselamatan Dan Kesehatan PenerbanganDedy SavradinataNessuna valutazione finora
- DVT NotesDocumento3 pagineDVT NotesTodd EvansNessuna valutazione finora