Potrebbero piacerti anche
- SDH Customized NQAS Checklists TN 27.12.2021Documento165 pagineSDH Customized NQAS Checklists TN 27.12.2021saravananNessuna valutazione finora
- 2021-22 Caddo Strong Start 2.0 Procedures and ProtocolsDocumento25 pagine2021-22 Caddo Strong Start 2.0 Procedures and ProtocolsCurtis HeyenNessuna valutazione finora
- National Association of The Deaf LawsuitDocumento27 pagineNational Association of The Deaf LawsuitWJLA-TV100% (1)
- Assessment of Hygiene Promotion in Madagascar - 2009Documento66 pagineAssessment of Hygiene Promotion in Madagascar - 2009HayZara MadagascarNessuna valutazione finora
- Ao2021 0045Documento14 pagineAo2021 0045che_c812125Nessuna valutazione finora
- Findings From Arnold Ventures' Request For Information On The Dual-Eligible ExperienceDocumento10 pagineFindings From Arnold Ventures' Request For Information On The Dual-Eligible ExperienceArnold VenturesNessuna valutazione finora
- President Cyril Ramaphosa Announces Move To Lockdown Level 3Documento11 paginePresident Cyril Ramaphosa Announces Move To Lockdown Level 3CityPressNessuna valutazione finora
- Kayakalp AwardsDocumento29 pagineKayakalp AwardsSwayam MohapatraNessuna valutazione finora
- Ulster County Guidance For Reopening Schools, 3-11-21Documento4 pagineUlster County Guidance For Reopening Schools, 3-11-21Daily FreemanNessuna valutazione finora
- Effects of COVID 19 Upon EMS Responses and Reporting in AlabamaDocumento77 pagineEffects of COVID 19 Upon EMS Responses and Reporting in AlabamaABC 33/40Nessuna valutazione finora
- Aol'S Wellbaby Program: An Employer Case StudyDocumento8 pagineAol'S Wellbaby Program: An Employer Case StudyAshish NemaNessuna valutazione finora
- Background: Livelihood Impacts of A Community-Led Total Sanitation Approach in KenyaDocumento6 pagineBackground: Livelihood Impacts of A Community-Led Total Sanitation Approach in Kenyaibrahim100% (1)
- SITXFSA005 Assessment Task 2 v.1.2.3 - 2024Documento17 pagineSITXFSA005 Assessment Task 2 v.1.2.3 - 2024Jorge CamachoNessuna valutazione finora
- Service Learning ProjectDocumento12 pagineService Learning Projectapi-260974225Nessuna valutazione finora
- Stroke Survivor Caregivers' Burden and Coping: Qualitative StudyDocumento25 pagineStroke Survivor Caregivers' Burden and Coping: Qualitative StudyNorulmumtazah JoharNessuna valutazione finora
- Reta ZetonewDocumento2 pagineReta Zetonewapi-598481829Nessuna valutazione finora
- Who Hand Hygiene Observation MethodDocumento8 pagineWho Hand Hygiene Observation MethodHandriyato SukmaNessuna valutazione finora
- Agricultural Extension in Vietnam: Its Roles, Problems and OpportunitiesDocumento7 pagineAgricultural Extension in Vietnam: Its Roles, Problems and OpportunitiesSANDITHA SETYA WISAKSANTINessuna valutazione finora
- Disaster Management - VaibhavDocumento27 pagineDisaster Management - Vaibhavvaibhav bhardwajNessuna valutazione finora
- Memo From NYU Administration To Board of TrusteesDocumento17 pagineMemo From NYU Administration To Board of TrusteesZoë SchlangerNessuna valutazione finora
- Adm of Oral Medication-Sep 08 - Edited 3 Dec 2008Documento11 pagineAdm of Oral Medication-Sep 08 - Edited 3 Dec 2008myvi31775% (4)
- People, Places, PossibilitiesDocumento64 paginePeople, Places, PossibilitiesThe Centre for Welfare ReformNessuna valutazione finora
- Liberal Platform March 2023Documento52 pagineLiberal Platform March 2023The GuardianNessuna valutazione finora
- Infection Control RevisedDocumento89 pagineInfection Control RevisedKWIZERA TREASURENessuna valutazione finora
- People Should Avoid Junk FoodsDocumento4 paginePeople Should Avoid Junk FoodsShireen BatoolNessuna valutazione finora
- Addressing The Opioid Epidemic On BYU Campus Through CAPS-O ProgramDocumento34 pagineAddressing The Opioid Epidemic On BYU Campus Through CAPS-O Programapi-439502865Nessuna valutazione finora
- NV Health Response COVID19Documento5 pagineNV Health Response COVID19Riley Snyder100% (1)
- FypDocumento12 pagineFypddalielaNessuna valutazione finora
- Cornell StatementDocumento4 pagineCornell StatementNews10NBCNessuna valutazione finora
- Service Learning Project: Civics Name - Mr. PfluegerDocumento6 pagineService Learning Project: Civics Name - Mr. Pfluegerapi-420474744Nessuna valutazione finora
- COVID-19 Guidance For Operating Schools Safely 728838 7Documento3 pagineCOVID-19 Guidance For Operating Schools Safely 728838 7WXYZ-TV Channel 7 DetroitNessuna valutazione finora
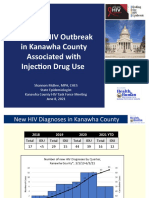
- Update: HIV Outbreak in Kanawha County Associated With Injection Drug UseDocumento10 pagineUpdate: HIV Outbreak in Kanawha County Associated With Injection Drug UseJune LefflerNessuna valutazione finora
- Ward 7 Progress Report 2022Documento12 pagineWard 7 Progress Report 2022Ward 7 Council OfficeNessuna valutazione finora
- JB Pritzker, Governor Ngozi O. Ezike, MD, Director: MemorandumDocumento2 pagineJB Pritzker, Governor Ngozi O. Ezike, MD, Director: MemorandumNewsTeam20Nessuna valutazione finora
- Topic 3 - Disease Control StrategiesDocumento25 pagineTopic 3 - Disease Control StrategiesKaey NiezamNessuna valutazione finora
- NoThing Left Behind Policy v5 PDFDocumento54 pagineNoThing Left Behind Policy v5 PDFO.r. Cadz100% (1)
- Marsh Farm Central Area Regeneration Masterplanning HIA SummaryDocumento42 pagineMarsh Farm Central Area Regeneration Masterplanning HIA SummarySalim VohraNessuna valutazione finora
- Shaka Drogho ResumeDocumento5 pagineShaka Drogho ResumeShama DolmaNessuna valutazione finora
- Anc Who 2019Documento68 pagineAnc Who 2019Pika LubisNessuna valutazione finora
- Nursing ResumeDocumento1 paginaNursing Resumeapi-508954625Nessuna valutazione finora
- Management of Osteomyelitis Oral SurgeryDocumento17 pagineManagement of Osteomyelitis Oral SurgeryFourthMolar.comNessuna valutazione finora
- Service Learning ProjectDocumento8 pagineService Learning Projectapi-211472021Nessuna valutazione finora
- Roadmap To The Revitalization: A Plan For Healthier and Sustainable CommunitiesDocumento14 pagineRoadmap To The Revitalization: A Plan For Healthier and Sustainable CommunitiesThe Press-Enterprise / pressenterprise.comNessuna valutazione finora
- Presidential Address On COVID-19 - 22. September 2021Documento12 paginePresidential Address On COVID-19 - 22. September 2021Daily Express NewsNessuna valutazione finora
- DMAS 7aDocumento2 pagineDMAS 7aBillie_anderson24730% (1)
- Patient Support AreasDocumento22 paginePatient Support AreasVivienne Rozenn LaytoNessuna valutazione finora
- Revised Project Narrative (11.28.2016) - Salesian Missions El SalvadorDocumento19 pagineRevised Project Narrative (11.28.2016) - Salesian Missions El SalvadorSilvia MendozaNessuna valutazione finora
- Factors Influencing Utilization of Prevention of Mother To Child Transmission (PMTCT) Services Among Pregnant Women Attending Ante-Natal ClinicDocumento6 pagineFactors Influencing Utilization of Prevention of Mother To Child Transmission (PMTCT) Services Among Pregnant Women Attending Ante-Natal ClinicIPROJECCT100% (1)
- 402ongsafety Spill CleanupDocumento147 pagine402ongsafety Spill CleanupShujaRehmanNessuna valutazione finora
- Metagonimus YokogawaiDocumento10 pagineMetagonimus Yokogawaiapi-341133750Nessuna valutazione finora
- Continuing Care Advisory Council (CCAC) Meeting MaterialsDocumento100 pagineContinuing Care Advisory Council (CCAC) Meeting MaterialsPhil AmmannNessuna valutazione finora
- Bioethical / Legal Issues About Nursing (RA 9173)Documento11 pagineBioethical / Legal Issues About Nursing (RA 9173)Richely MedezaNessuna valutazione finora
- Sdn-Cuban PolyclinicDocumento23 pagineSdn-Cuban PolyclinicMaria Socorro AlcantaraNessuna valutazione finora
- National Disaster Recovery Framework2nd 2Documento59 pagineNational Disaster Recovery Framework2nd 2Uloko ChristopherNessuna valutazione finora
- SCHD Investigation Final ReportDocumento9 pagineSCHD Investigation Final ReportFOX13 MemphisNessuna valutazione finora
- Response To Sunday Times April 12 2020Documento5 pagineResponse To Sunday Times April 12 2020Charles CilliersNessuna valutazione finora
- MOH CDC Draft Advert July 2023 2Documento7 pagineMOH CDC Draft Advert July 2023 2KevinNessuna valutazione finora
- In-Service Education VirginiaDocumento25 pagineIn-Service Education Virginiaapi-234162801Nessuna valutazione finora
- Grace Villa Inspection Report: Dec 11, 2020Documento3 pagineGrace Villa Inspection Report: Dec 11, 2020The Hamilton SpectatorNessuna valutazione finora
- 2020 Inclusiveness IndexDocumento55 pagine2020 Inclusiveness IndexHPR NewsNessuna valutazione finora
- 2021 Hawaii Physician Workforce AssessmentDocumento44 pagine2021 Hawaii Physician Workforce AssessmentHPR NewsNessuna valutazione finora
- Yukio Okutsu State Veterans Home - HI-EMA Report 9-11-2020 - REDACTEDDocumento6 pagineYukio Okutsu State Veterans Home - HI-EMA Report 9-11-2020 - REDACTEDHonolulu Star-AdvertiserNessuna valutazione finora
- Assessment & Priorities For The Health and Well-Being in Native Hawaiians and Pacific IslandersDocumento43 pagineAssessment & Priorities For The Health and Well-Being in Native Hawaiians and Pacific IslandersHPR News100% (1)
- The Perfect Storm 2021: Hawai I's Physician Shortage CrisisDocumento15 pagineThe Perfect Storm 2021: Hawai I's Physician Shortage CrisisHPR NewsNessuna valutazione finora
- Āina Kupuna Bill (Maui County)Documento3 pagineĀina Kupuna Bill (Maui County)HPR News100% (1)
- City Letter To HART Chief Procurement OfficerDocumento8 pagineCity Letter To HART Chief Procurement OfficerHPR NewsNessuna valutazione finora
- Mo'omomi CBSFA ProposalDocumento251 pagineMo'omomi CBSFA ProposalHPR NewsNessuna valutazione finora
- Making Hawaii Safe For Travel ABCDocumento23 pagineMaking Hawaii Safe For Travel ABCHPR NewsNessuna valutazione finora
- City and County of Honolulu vs. Sunoco LP Et AlDocumento119 pagineCity and County of Honolulu vs. Sunoco LP Et AlHPR NewsNessuna valutazione finora
- Honolulu's Second Stay at Home / Work From Home OrderDocumento16 pagineHonolulu's Second Stay at Home / Work From Home OrderHPR NewsNessuna valutazione finora
- Mayor Caldwell's Supplemental Proclamation March 18Documento3 pagineMayor Caldwell's Supplemental Proclamation March 18HPR NewsNessuna valutazione finora
- DOJ, Quarantine FilingDocumento21 pagineDOJ, Quarantine FilingHNNNessuna valutazione finora
- FY2021 Capital Improvements Budget ProposalDocumento587 pagineFY2021 Capital Improvements Budget ProposalHPR NewsNessuna valutazione finora
- DPP Permit Processing Final ReportDocumento112 pagineDPP Permit Processing Final ReportHPR NewsNessuna valutazione finora
- UHERO 2020 Q1 ForecastDocumento5 pagineUHERO 2020 Q1 ForecastHPR NewsNessuna valutazione finora
- U.S. Department of Justice Press Release On Arthur Brun IndictmentDocumento5 pagineU.S. Department of Justice Press Release On Arthur Brun IndictmentHPR NewsNessuna valutazione finora
- Mauna Kea Access Road LawsuitDocumento14 pagineMauna Kea Access Road LawsuitHPR NewsNessuna valutazione finora
- 2019-12-26 Letter To Noe Noe Wong Wilson Re Resolution To Open Maunakea Access RoadDocumento2 pagine2019-12-26 Letter To Noe Noe Wong Wilson Re Resolution To Open Maunakea Access RoadHPR NewsNessuna valutazione finora
- FY2021 Operating Budget ProposalDocumento399 pagineFY2021 Operating Budget ProposalHPR NewsNessuna valutazione finora
- DHHL Acquisition of Mō Ili Ili PropertiesDocumento6 pagineDHHL Acquisition of Mō Ili Ili PropertiesHPR NewsNessuna valutazione finora
- DPP Permit Processing Final ReportDocumento112 pagineDPP Permit Processing Final ReportHPR NewsNessuna valutazione finora
- State of The StateDocumento11 pagineState of The StateHNNNessuna valutazione finora
- Hawaii Migration Flows 2013-2017 ReportDocumento41 pagineHawaii Migration Flows 2013-2017 ReportHPR NewsNessuna valutazione finora
- YWomenVote-Report FNL 12-11-19Documento32 pagineYWomenVote-Report FNL 12-11-19HPR NewsNessuna valutazione finora
- YWCA YWomenVoteExecSummaryDocumento2 pagineYWCA YWomenVoteExecSummaryHPR NewsNessuna valutazione finora
- Tulsi GabbardDocumento4 pagineTulsi GabbardHPR NewsNessuna valutazione finora
- 12-24 Doctor ShortageDocumento18 pagine12-24 Doctor ShortageHawaii News NowNessuna valutazione finora
- GM 30thleg Supplemental Budget FB 2019 21Documento15 pagineGM 30thleg Supplemental Budget FB 2019 21HPR NewsNessuna valutazione finora
- Essential Safety Requirements - (Esr) Standards For Saudi Cbahi Accreditation in Hospitals and Phc'S. Gdharr Riyadh Saudi ArabiaDocumento36 pagineEssential Safety Requirements - (Esr) Standards For Saudi Cbahi Accreditation in Hospitals and Phc'S. Gdharr Riyadh Saudi Arabiarelena badr100% (1)
- DHA Health Facility Guidelines 2019: Part B - Health Facility Briefing & Design 430 - Waste Management UnitDocumento24 pagineDHA Health Facility Guidelines 2019: Part B - Health Facility Briefing & Design 430 - Waste Management UnitMaherNessuna valutazione finora
- Delian Catalogue - Hi - Lite 2 - CHECKED PDFDocumento84 pagineDelian Catalogue - Hi - Lite 2 - CHECKED PDFAnonymous KZQ8MGNessuna valutazione finora
- Thesis Report PDFDocumento73 pagineThesis Report PDFSherly IreneNessuna valutazione finora
- 4621 NYI Exam BlueprintDocumento4 pagine4621 NYI Exam BlueprintjelenabasaNessuna valutazione finora
- Ccu Deparmental Operation PoliciesDocumento7 pagineCcu Deparmental Operation PoliciesamalfarhanaNessuna valutazione finora
- Infection Control Practice On Vital Signs Equipment: A Survey Among Senior Nursing Students in Iloilo City, PhilippinesDocumento7 pagineInfection Control Practice On Vital Signs Equipment: A Survey Among Senior Nursing Students in Iloilo City, PhilippinesRyan Michael OducadoNessuna valutazione finora
- National Guidelines For IPC in HCF - Final PDFDocumento264 pagineNational Guidelines For IPC in HCF - Final PDFGorav BhallaNessuna valutazione finora
- Manual of in Dental Settings: Infection Prevention & ControlDocumento134 pagineManual of in Dental Settings: Infection Prevention & Controlsamarcullen100% (1)
- RR 5417Documento144 pagineRR 5417Handriyato SukmaNessuna valutazione finora
- Swaziland Striving For Freedom Vol 38 Apr To June 2020Documento96 pagineSwaziland Striving For Freedom Vol 38 Apr To June 2020Richard RooneyNessuna valutazione finora
- Jcia QaDocumento84 pagineJcia Qahegdeshailu50% (4)
- Infection Prevention and Control Guideline For Flexible Gastrointestinal Endoscopy and Flexible Bronchoscopy - Public Health Agency of CanadaDocumento21 pagineInfection Prevention and Control Guideline For Flexible Gastrointestinal Endoscopy and Flexible Bronchoscopy - Public Health Agency of CanadaJuan Vicente Reyes LimaNessuna valutazione finora
- HIV and Dental Treatment: JSM DentistryDocumento6 pagineHIV and Dental Treatment: JSM DentistryMuhamad RamadanNessuna valutazione finora
- Hospital Possible Interview Questions-2Documento13 pagineHospital Possible Interview Questions-2Herbalife-Slabeste Sanatos Speranta100% (1)
- Managing COVID-19 in Low-And Middle-Income Countries: The Public Health ResponseDocumento2 pagineManaging COVID-19 in Low-And Middle-Income Countries: The Public Health ResponseNuzlaNessuna valutazione finora
- The Nhsscotland National Cleaning Services Specification: Healthcare Associated Infection Task ForceDocumento119 pagineThe Nhsscotland National Cleaning Services Specification: Healthcare Associated Infection Task ForcedidikNessuna valutazione finora
- Clinical Practice Guideline For An Infection Controlexposure Control Program in The Oral Healthcare SettingDocumento1 paginaClinical Practice Guideline For An Infection Controlexposure Control Program in The Oral Healthcare Settingapi-399847495Nessuna valutazione finora
- The Principles of Infection Prevention and ControlDocumento25 pagineThe Principles of Infection Prevention and ControlRamona Lazurca100% (1)
- Infection Control On Linen and Laundry ManagementDocumento46 pagineInfection Control On Linen and Laundry ManagementRosafe E. Peralta100% (3)
- DIN 1946-4 Engl. Dez. 2008Documento68 pagineDIN 1946-4 Engl. Dez. 2008Lệ HoaNessuna valutazione finora
- Chemotherapy Leukemia: B. Administer Varicella-Zoster Immune Globulin To The ClientDocumento12 pagineChemotherapy Leukemia: B. Administer Varicella-Zoster Immune Globulin To The ClientAsterlyn ConiendoNessuna valutazione finora
- Pdca HHDocumento5 paginePdca HHFaozan FikriNessuna valutazione finora
- Defects of Farm Tool and RemediesDocumento5 pagineDefects of Farm Tool and RemediesAbela Jazen Jacob100% (1)
- Statement of Deficiencies and Plan of Correction 8/10/2020Documento32 pagineStatement of Deficiencies and Plan of Correction 8/10/2020Maine Trust For Local NewsNessuna valutazione finora
- 0 - MDI-P (Precursor ASEA) - Studiu Efect Germeni Agresivi - Baltch 2000Documento7 pagine0 - MDI-P (Precursor ASEA) - Studiu Efect Germeni Agresivi - Baltch 2000andrushkkutzaNessuna valutazione finora
- PROCEDURESSSSSSSDocumento206 paginePROCEDURESSSSSSSJosie CalunsagNessuna valutazione finora
- Planning An Operation Theatre ComplexDocumento4 paginePlanning An Operation Theatre ComplexRaviraj PisheNessuna valutazione finora
- SCALERDocumento168 pagineSCALERDaniel Parada VanegasNessuna valutazione finora
- UNIT PLAN - TRENDS IN MEDCAL SURGICAL NURSING BY Gunjan RawalDocumento14 pagineUNIT PLAN - TRENDS IN MEDCAL SURGICAL NURSING BY Gunjan Rawalgunjan100% (1)
- A Complete Guide to Safety Officer Interview Questions and AnswersDa EverandA Complete Guide to Safety Officer Interview Questions and AnswersValutazione: 4 su 5 stelle4/5 (1)
- Practical Industrial Safety, Risk Assessment and Shutdown SystemsDa EverandPractical Industrial Safety, Risk Assessment and Shutdown SystemsValutazione: 4 su 5 stelle4/5 (11)
- Rules of Thumb for Maintenance and Reliability EngineersDa EverandRules of Thumb for Maintenance and Reliability EngineersValutazione: 4.5 su 5 stelle4.5/5 (12)
- Workbook to Accompany Maintenance & Reliability Best PracticesDa EverandWorkbook to Accompany Maintenance & Reliability Best PracticesValutazione: 3.5 su 5 stelle3.5/5 (3)
- Guidelines for Auditing Process Safety Management SystemsDa EverandGuidelines for Auditing Process Safety Management SystemsNessuna valutazione finora
- Handbook of Fire and Explosion Protection Engineering Principles: for Oil, Gas, Chemical and Related FacilitiesDa EverandHandbook of Fire and Explosion Protection Engineering Principles: for Oil, Gas, Chemical and Related FacilitiesValutazione: 4.5 su 5 stelle4.5/5 (2)
- Healthy Buildings: How Indoor Spaces Drive Performance and ProductivityDa EverandHealthy Buildings: How Indoor Spaces Drive Performance and ProductivityValutazione: 5 su 5 stelle5/5 (2)
- Guidelines for Initiating Events and Independent Protection Layers in Layer of Protection AnalysisDa EverandGuidelines for Initiating Events and Independent Protection Layers in Layer of Protection AnalysisValutazione: 5 su 5 stelle5/5 (1)
- Functional Safety from Scratch: A Practical Guide to Process Industry ApplicationsDa EverandFunctional Safety from Scratch: A Practical Guide to Process Industry ApplicationsNessuna valutazione finora
- Chemical Process Safety: Learning from Case HistoriesDa EverandChemical Process Safety: Learning from Case HistoriesValutazione: 4 su 5 stelle4/5 (14)
- Plutopia: Nuclear Families, Atomic Cities, and the Great Soviet and American Plutonium DisastersDa EverandPlutopia: Nuclear Families, Atomic Cities, and the Great Soviet and American Plutonium DisastersValutazione: 4 su 5 stelle4/5 (32)
- The ISO 45001:2018 Implementation Handbook: Guidance on Building an Occupational Health and Safety Management SystemDa EverandThe ISO 45001:2018 Implementation Handbook: Guidance on Building an Occupational Health and Safety Management SystemNessuna valutazione finora
- The Invisible Rainbow: A History of Electricity and LifeDa EverandThe Invisible Rainbow: A History of Electricity and LifeValutazione: 4.5 su 5 stelle4.5/5 (21)
- Tensor Technology Guide: Tensor Ring Benefits and UsesDa EverandTensor Technology Guide: Tensor Ring Benefits and UsesValutazione: 5 su 5 stelle5/5 (2)
- Nutritional and Therapeutic Interventions for Diabetes and Metabolic SyndromeDa EverandNutritional and Therapeutic Interventions for Diabetes and Metabolic SyndromeNessuna valutazione finora
- A Poison Like No Other: How Microplastics Corrupted Our Planet and Our BodiesDa EverandA Poison Like No Other: How Microplastics Corrupted Our Planet and Our BodiesValutazione: 5 su 5 stelle5/5 (1)
- Environmental and Health and Safety Management: A Guide to ComplianceDa EverandEnvironmental and Health and Safety Management: A Guide to ComplianceValutazione: 4 su 5 stelle4/5 (2)
- General Orders for Security Personnel: A Guide to Maintaining Discipline and ProfessionalismDa EverandGeneral Orders for Security Personnel: A Guide to Maintaining Discipline and ProfessionalismNessuna valutazione finora
- Establishing an occupational health & safety management system based on ISO 45001Da EverandEstablishing an occupational health & safety management system based on ISO 45001Valutazione: 4 su 5 stelle4/5 (5)
- Epidemiology and Demography in Public HealthDa EverandEpidemiology and Demography in Public HealthJaphet KillewoValutazione: 5 su 5 stelle5/5 (1)
- Handbook of Hazardous Chemical PropertiesDa EverandHandbook of Hazardous Chemical PropertiesValutazione: 5 su 5 stelle5/5 (1)
- Safety Fundamentals and Best Practices in Construction IndustryDa EverandSafety Fundamentals and Best Practices in Construction IndustryNessuna valutazione finora